

Giant scalp melanoma: a case report and review of the literature
- PMID: 23185647
- PMCID: PMC3501267
Giant scalp melanoma: a case report and review of the literature
Abstract
Introduction: Among malignant melanoma lesions, those occurring on the scalp and neck have a particularly poor prognosis. In this case report, we present the largest melanoma of the head and neck and one of the largest melanomas of any anatomic site reported in the literature to date.
Methods: The biopsy revealed left scalp melanoma with a Breslow's thickness of at least 14 mm, and final needle aspiration of lymphadenopathy was consistent with malignant melanoma. Preoperative staging was T4aN3Mx. Wide local excision with 3-cm margins was performed, which included excision of the left ear en-bloc, along with a selective left neck dissection. Reconstruction was performed with a Bilayer Wound Matrix (Integra, 311 Enterprise Drive, Plainsboro, New Jersey) and eventual thin split-thickness skin graft.
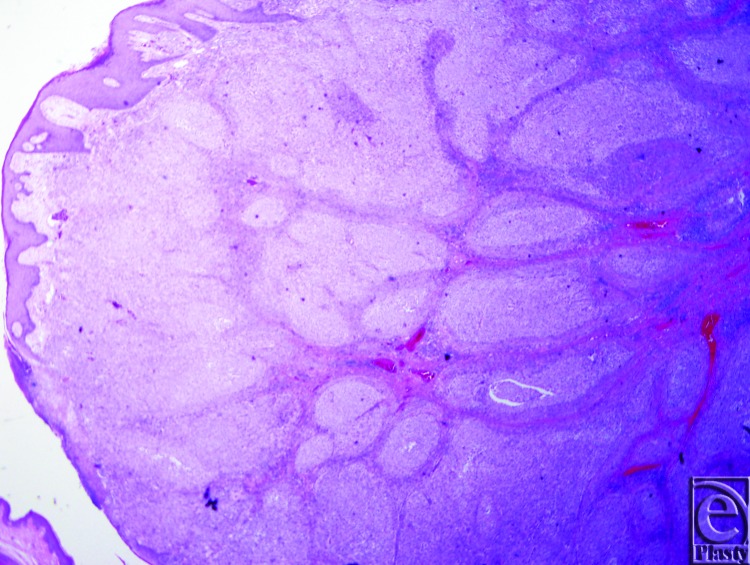
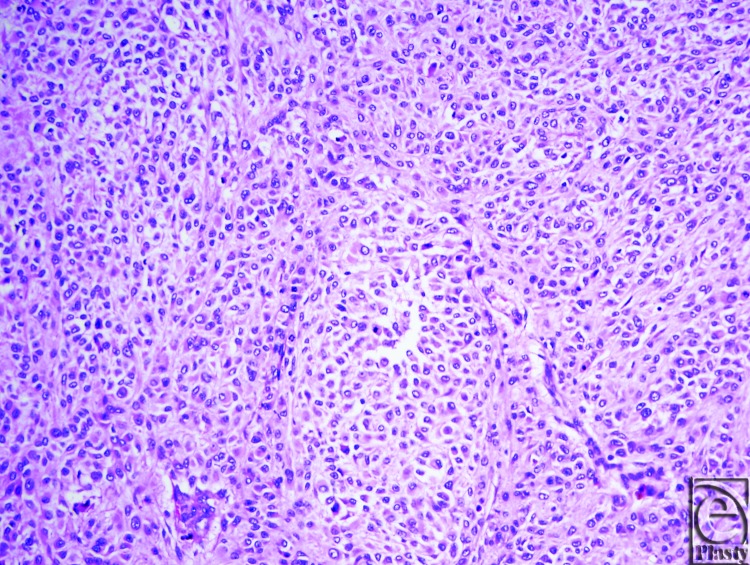
Results: Final pathology of the left scalp en-bloc excision was a 14.5 × 10.4 cm malignant melanoma, Breslow's thickness of 18 mm. Numerous lymph nodes were positive for melanoma as well. Final pathologic staging was determined to be T4b N3 M1, Stage IV. Later the patient underwent split-thickness skin graft placement on the left scalp acellular dermal matrix, which healed with complete graft take.
Discussion: This case report demonstrates a unique presentation of a giant melanoma. With few other cases reported for comparison, it appears our patient's prognosis is poor, despite treatment according to current guidelines.
Figures


Similar articles
-
Management of skin defect following resection of Stage IV scalp melanoma: A case report.Int J Surg Case Rep. 2016;29:8-10. doi: 10.1016/j.ijscr.2016.10.027. Epub 2016 Oct 17. Int J Surg Case Rep. 2016. PMID: 27810611 Free PMC article.
-
Prognostic factors in head and neck melanoma. Effect of lesion location.Cancer. 1988 Aug 15;62(4):831-7. doi: 10.1002/1097-0142(19880815)62:4<831::aid-cncr2820620432>3.0.co;2-x. Cancer. 1988. PMID: 3395962
-
Value of anatomic site, histology and clinicopathological parameters for prediction of lymph node metastasis and overall survival in head and neck melanomas.J Craniomaxillofac Surg. 2014 Jul;42(5):e252-8. doi: 10.1016/j.jcms.2013.09.007. Epub 2013 Oct 7. J Craniomaxillofac Surg. 2014. PMID: 24216129
-
Malignant melanoma in the lower extremity. A comprehensive overview.Clin Podiatr Med Surg. 1986 Jul;3(3):533-50. Clin Podiatr Med Surg. 1986. PMID: 2943398 Review.
-
Current concepts in the management of patients with melanoma.Am J Clin Dermatol. 2002;3(6):401-26. doi: 10.2165/00128071-200203060-00004. Am J Clin Dermatol. 2002. PMID: 12113649 Review.
Cited by
-
Advanced Presentation of Homeopathically treated Giant Melanoma: A Case Report.J Clin Aesthet Dermatol. 2019 Jan;12(1):28-31. Epub 2019 Jan 1. J Clin Aesthet Dermatol. 2019. PMID: 30881574 Free PMC article.
-
A Unique Case of Late Presentation Giant Lower Extremity Malignant Melanoma.Cureus. 2024 Mar 2;16(3):e55414. doi: 10.7759/cureus.55414. eCollection 2024 Mar. Cureus. 2024. PMID: 38567210 Free PMC article.
-
Case Report and Literature Review of Giant Cutaneous Malignant Melanoma: What's Keeping Patients Away?Eplasty. 2022 Sep 23;22:e45. eCollection 2022. Eplasty. 2022. PMID: 36212603 Free PMC article.
-
Giant malignant melanoma of the upper limb: a case report and review of the literature.J Med Case Rep. 2025 May 18;19(1):234. doi: 10.1186/s13256-025-05303-1. J Med Case Rep. 2025. PMID: 40383796 Free PMC article. Review.
-
Unusual Presentation of Giant Upper Limb Malignant Melanoma.Cureus. 2021 Aug 8;13(8):e16996. doi: 10.7759/cureus.16996. eCollection 2021 Aug. Cureus. 2021. PMID: 34540398 Free PMC article.
References
-
- Lachiewicz AM, Berwick M, Wiggins CL, Thomas NE. Survival differences between patients with scalp or neck melanoma and those with melanoma of other sites in the Surveillance, Epidemiology, and End Results (SEER) program. Arch Dermatol. 2008;144(4):515–21. - PubMed
-
- Leong SP, Accortt NA, Essner R, et al. Impact of sentinel node status and other risk factors on the clinical outcome of head and neck melanoma patients. Arch Otolaryngol Head Neck Surg. 2006;132(4):370–3. - PubMed
-
- Grisham AD. Giant melanoma: novel problem, same approach. South Med J. 2010;103(11):1161–2. - PubMed
-
- Panajotovic L, Dordevic B, Pavlovic MD. A giant primary cutaneous melanoma of the scalp—can it be that big? J Eur Acad Dermatol Venereol. 2007;21(10):1417–8. - PubMed
-
- del Boz J, Garcia JM, Martinez S, Gomez M. Giant melanoma and depression. Am J Clin Dermatol. 2009;10(6):419–20. - PubMed
LinkOut - more resources
Full Text Sources
Research Materials