

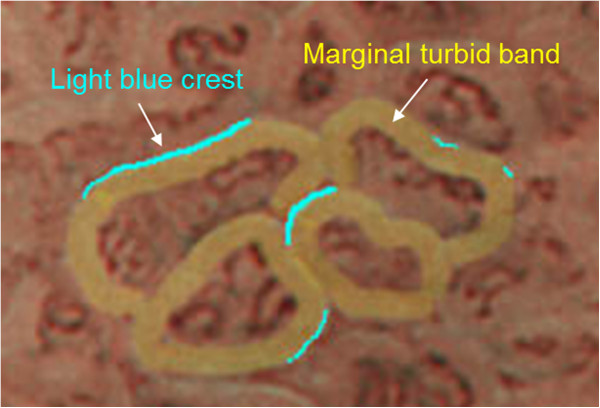
Marginal turbid band and light blue crest, signs observed in magnifying narrow-band imaging endoscopy, are indicative of gastric intestinal metaplasia
- PMID: 23185997
- PMCID: PMC3543218
- DOI: 10.1186/1471-230X-12-169
Marginal turbid band and light blue crest, signs observed in magnifying narrow-band imaging endoscopy, are indicative of gastric intestinal metaplasia
Abstract
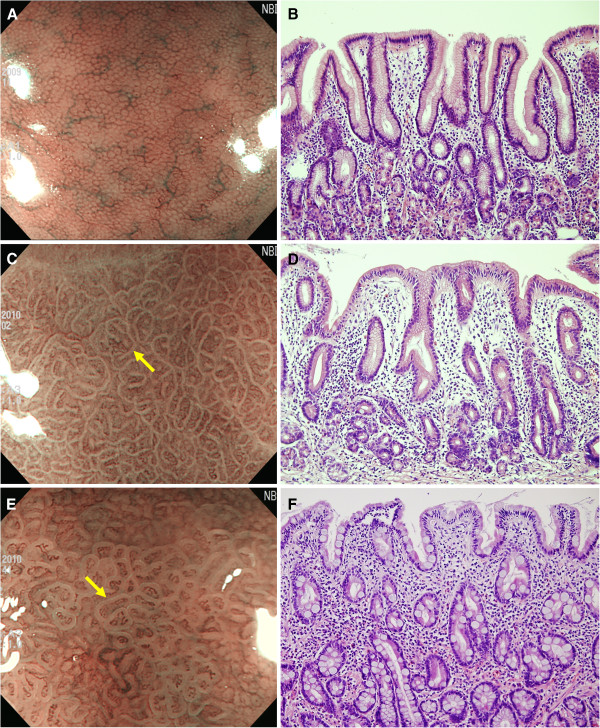
Background: Gastric intestinal metaplasia (IM) usually appears in flat mucosa and shows few morphologic changes, making diagnosis using conventional endoscopy unreliable. Magnifying narrow-band imaging (NBI) endoscopy enables evaluation of detailed morphological features that correspond with the underlying histology. The aim of this study was to investigate and clarify the diagnostic efficacy of magnifying NBI endoscopic findings for the prediction and diagnosis of IM.
Methods: Forty-seven patients were prospectively enrolled, and magnifying NBI examinations were performed in the lesser curvature of the midbody and the greater curvature of the upper body. The marginal turbid band (MTB) was defined as an enclosing white turbid band on the epithelial surface/gyri; light blue crest (LBC), as a fine, blue-white line on the crest of the epithelial surface/gyri. Immediately after observation under magnifying endoscopy, biopsy specimens were obtained from the evaluated areas.
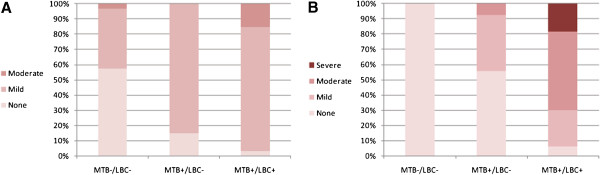
Results: The degree of IM significantly increased with increasing MTB/LBC positivity (MTB(-)/LBC(-), 0.00 ± 0.00; MTB(+)/LBC(-), 0.44 ± 0.51; MTB(+)/LBC(+), 0.94 ± 0.24; p < 0.001). Moderate-to-severe IM was more common in MTB(+)/LBC(+) areas than in MTB(+)/LBC(-) areas (p < 0.001). For the diagnosis of IM, MTB had a sensitivity, specificity, and accuracy of 100%, 66.0%, and 81.7%, respectively, and the corresponding values for LBC were 72.1%, 96.0%, and 84.9%.
Conclusion: MTB and LBC observed in the gastric mucosa with magnifying NBI endoscopy are highly accurate indicators of the presence of IM. MTB likely represents a sign of early gastric IM, while LBC appears with progression to severe IM.
Figures
References
-
- Correa P. A human model of gastric carcinogenesis. Cancer Res. 1988;48(13):3554–3560. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
