

Gastric bypass and banding equally improve insulin sensitivity and β cell function
- PMID: 23187122
- PMCID: PMC3512168
- DOI: 10.1172/JCI64895
Gastric bypass and banding equally improve insulin sensitivity and β cell function
Abstract
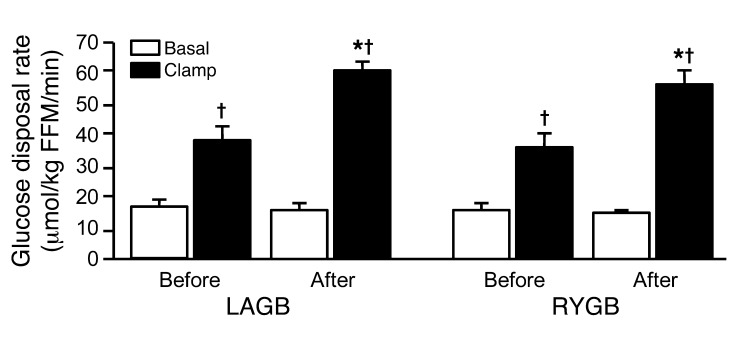
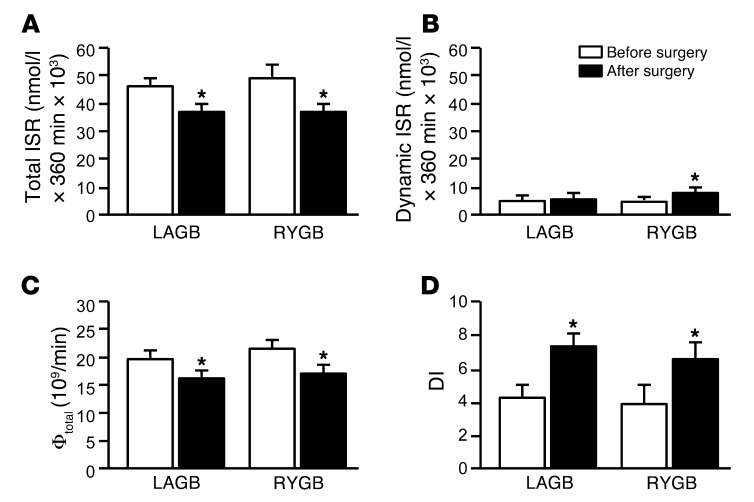
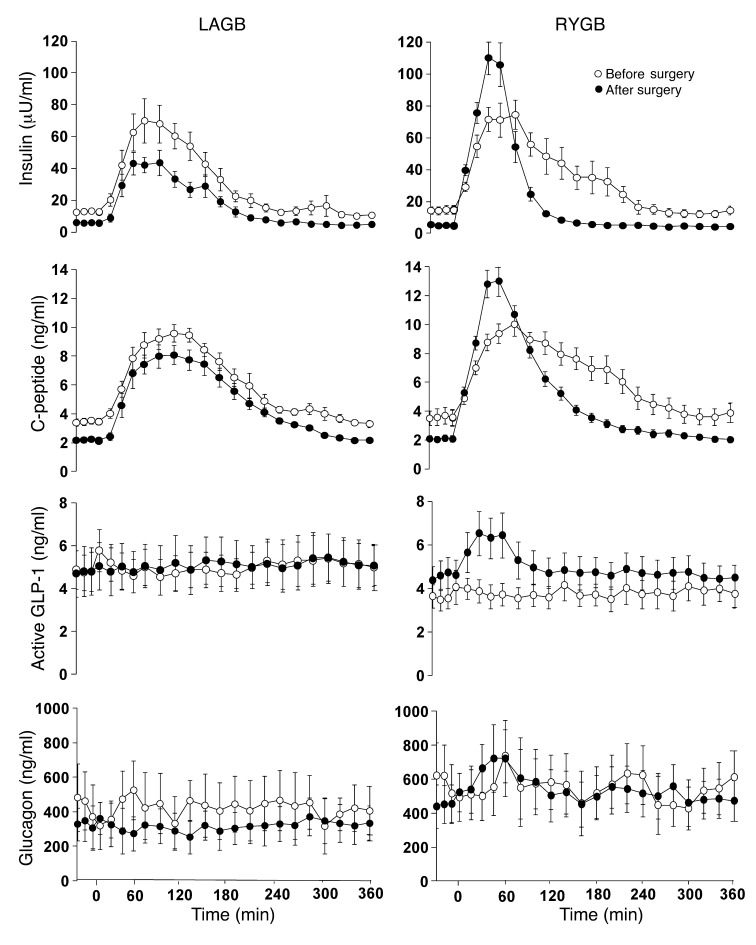
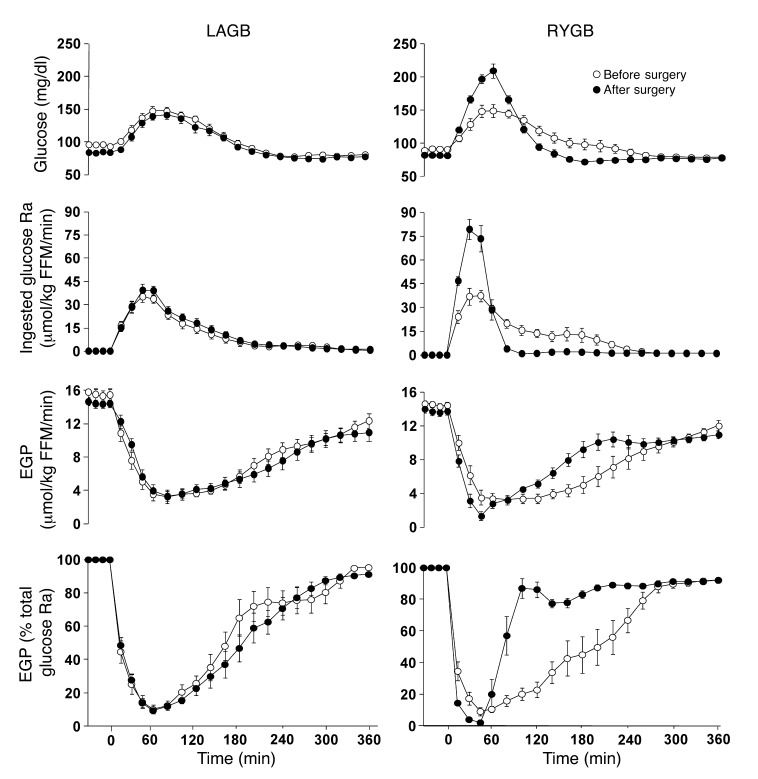
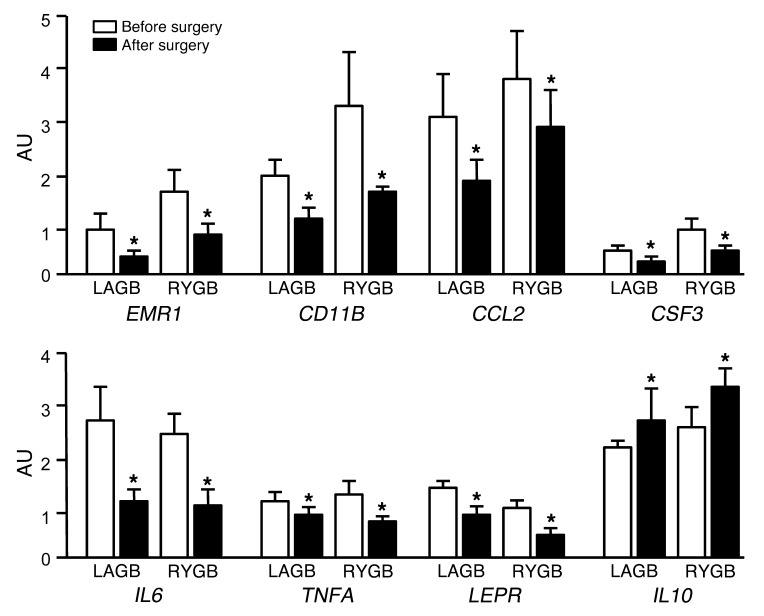
Bariatric surgery in obese patients is a highly effective method of preventing or resolving type 2 diabetes mellitus (T2DM); however, the remission rate is not the same among different surgical procedures. We compared the effects of 20% weight loss induced by laparoscopic adjustable gastric banding (LAGB) or Roux-en-Y gastric bypass (RYGB) surgery on the metabolic response to a mixed meal, insulin sensitivity, and β cell function in nondiabetic obese adults. The metabolic response to meal ingestion was markedly different after RYGB than after LAGB surgery, manifested by rapid delivery of ingested glucose into the systemic circulation, by an increase in the dynamic insulin secretion rate, and by large, early postprandial increases in plasma glucose, insulin, and glucagon-like peptide-1 concentrations in the RYGB group. However, the improvement in oral glucose tolerance, insulin sensitivity, and overall β cell function after weight loss were not different between surgical groups. Additionally, both surgical procedures resulted in a similar decrease in adipose tissue markers of inflammation. We conclude that marked weight loss itself is primarily responsible for the therapeutic effects of RYGB and LAGB on insulin sensitivity, β cell function, and oral glucose tolerance in nondiabetic obese adults.
Figures
References
-
- Niskanen L, Uusitupa M, Sarlund H, Siitonen O, Paljarvi L, Laakso M. The effects of weight loss on insulin sensitivity, skeletal muscle composition and capillary density in obese non-diabetic subjects. Int J Obes Relat Metab Disord. 1996;20(2):154–160. - PubMed
-
- Guldstrand M, Ahren B, Adamson U. Improved beta-cell function after standardized weight reduction in severely obese subjects. Am J Physiol Endocrinol Metab. 2003;284(3):E557–E565. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
