

Outcomes of antiretroviral therapy in children in Asia and Africa: a comparative analysis of the IeDEA pediatric multiregional collaboration
- PMID: 23187940
- PMCID: PMC3556242
- DOI: 10.1097/QAI.0b013e31827b70bf
Outcomes of antiretroviral therapy in children in Asia and Africa: a comparative analysis of the IeDEA pediatric multiregional collaboration
Abstract
Background: We investigated 18-month incidence and determinants of death and loss to follow-up of children after antiretroviral therapy (ART) initiation in a multiregional collaboration in lower-income countries.
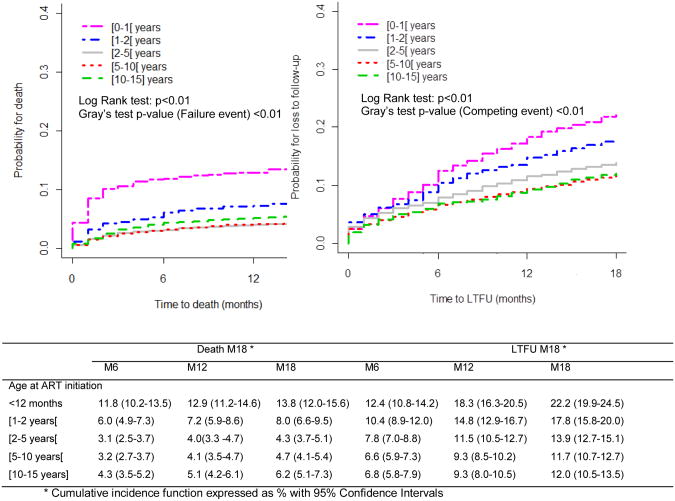
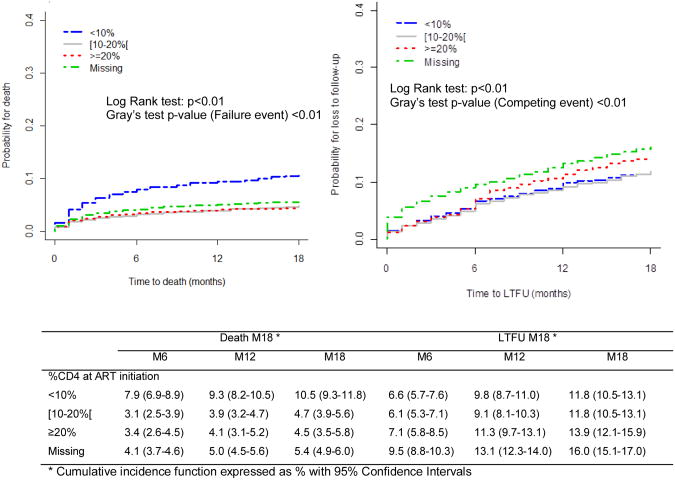
Methods: HIV-infected children (positive polymerase chain reaction <18 months or positive serology ≥18 months) from International Epidemiologic Databases to Evaluate AIDS cohorts, <16 years, initiating ART were eligible. A competing risk regression model was used to analyze the independent risk of 2 failure types: death and loss to follow-up (>6 months).
Findings: Data on 13,611 children, from Asia (N = 1454), East Africa (N = 3114), Southern Africa (N = 6212), and West Africa (N = 2881) contributed 20,417 person-years of follow-up. At 18 months, the adjusted risk of death was 4.3% in East Africa, 5.4% in Asia, 5.7% in Southern Africa, and 7.4% in West Africa (P = 0.01). Age < 24 months, World Health Organization stage 4, CD4 < 10%, attending a private sector clinic, larger cohort size, and living in West Africa were independently associated with poorer survival. The adjusted risk of loss to follow-up was 4.1% in Asia, 9.0% in Southern Africa, 14.0% in East Africa, and 21.8% in West Africa (P < 0.01). Age < 12 months, nonnucleoside reverse transcriptase inhibitor I-based ART regimen, World Health Organization stage 4 at ART start, ART initiation after 2005, attending a public sector or a nonurban clinic, having to pay for laboratory tests or antiretroviral drugs, larger cohort size, and living in East Africa or West Africa were significantly associated with higher loss to follow-up.
Conclusions: Findings differed substantially across regions but raise overall concerns about delayed ART start, low access to free HIV services for children, and increased workload on program retention in lower-income countries. Universal free access to ART services and innovative approaches are urgently needed to improve pediatric outcomes at the program level.
Conflict of interest statement
Figures
Comment in
-
Toward an AIDS-free generation with option B+: reconceptualizing and integrating prevention of mother to child transmission (PMTCT) with pediatric antiretroviral therapy initiatives.J Acquir Immune Defic Syndr. 2013 Feb 1;62(2):127-8. doi: 10.1097/QAI.0b013e3182749994. J Acquir Immune Defic Syndr. 2013. PMID: 23018370 No abstract available.
References
-
- World Health Organisation, UNAIDS, Unicef. Global HIV/AIDS Response: Epidemic update and health sector progress towards Universal Access, Progress Report 2011. Geneva: WHO, UNAIDS, Unicef; 2011.
-
- O'Brien DP, Sauvageot D, Zachariah R, Humblet P. In resource-limited settings good early outcomes can be achieved in children using adult fixed-dose combination antiretroviral therapy. AIDS. 2006 Oct 3;20(15):1955–60. - PubMed
-
- UNAIDS. Unaids report on the global AIDS epidemic 2010. Geneva: UNAIDS; 2010. Global report.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
