

Predictive accuracy of the Veterans Aging Cohort Study index for mortality with HIV infection: a North American cross cohort analysis
- PMID: 23187941
- PMCID: PMC3619393
- DOI: 10.1097/QAI.0b013e31827df36c
Predictive accuracy of the Veterans Aging Cohort Study index for mortality with HIV infection: a North American cross cohort analysis
Abstract
Background: By supplementing an index composed of HIV biomarkers and age (restricted index) with measures of organ injury, the Veterans Aging Cohort Study (VACS) index more completely reflects risk of mortality. We compare the accuracy of the VACS and restricted indices (1) among subjects outside the Veterans Affairs Healthcare System, (2) more than 1-5 years of prior exposure to antiretroviral therapy (ART), and (3) within important patient subgroups.
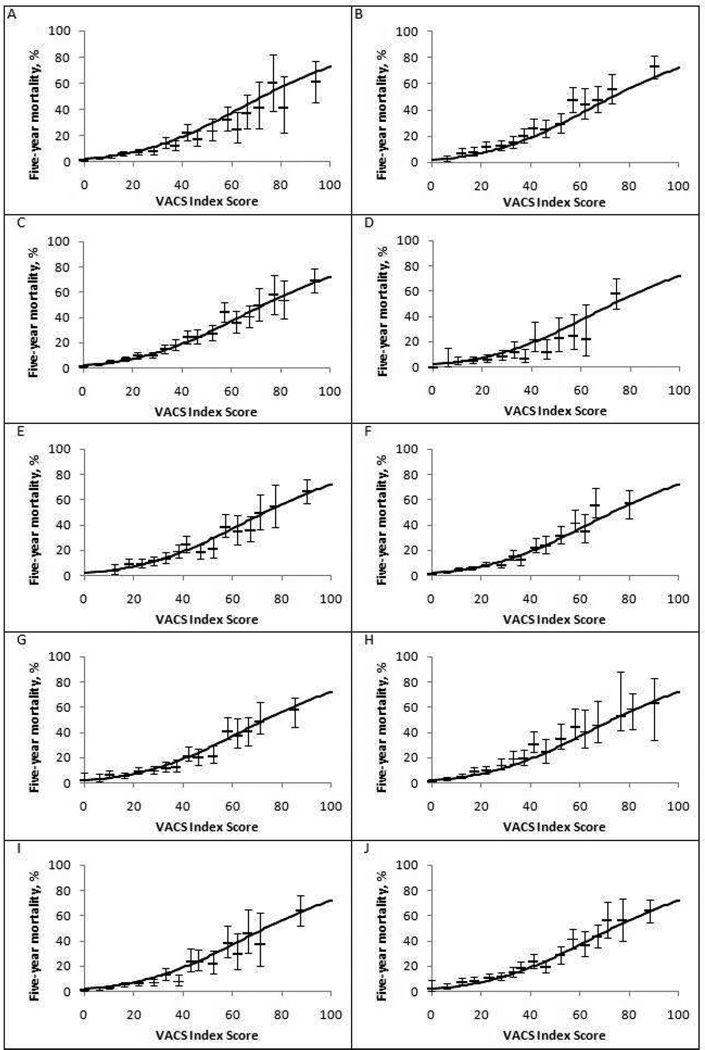
Methods: We used data from 13 cohorts in the North American AIDS Cohort Collaboration (n = 10, 835) limiting analyses to HIV-infected subjects with at least 12 months exposure to ART. Variables included demographic, laboratory (CD4 count, HIV-1 RNA, hemoglobin, platelets, aspartate and alanine transaminase, creatinine, and hepatitis C status), and survival. We used C-statistics and net reclassification improvement (NRI) to test discrimination varying prior ART exposure from 1 to 5 years. We then combined Veterans Affairs Healthcare System (n = 5066) and North American AIDS Cohort Collaboration data, fit a parametric survival model, and compared predicted to observed mortality by cohort, gender, age, race, and HIV-1 RNA level.
Results: Mean follow-up was 3.3 years (655 deaths). Compared with the restricted index, the VACS index showed greater discrimination (C-statistics: 0.77 vs. 0.74; NRI: 12%; P < 0.0001). NRI was highest among those with HIV-1 RNA <500 copies per milliliter (25%) and age ≥50 years (20%). Predictions were similar to observed mortality among all subgroups.
Conclusions: VACS index scores discriminate risk and translate into accurate mortality estimates over 1-5 years of exposure to ART and for diverse patient subgroups from North American.
Conflict of interest statement
Figures


References
-
- D'Arminio MA, Sabin CA, Phillips A, Sterne J, May M, Justice A, Dabis F, Grabar S, Ledergerber B, Gill J, Reiss P, Egger M. The changing incidence of AIDS events in patients receiving highly active antiretroviral therapy. Arch Intern Med. 2005;165:416–423. - PubMed
-
- Losina E, Schackman BR, Sadownik SN, Gebo KA, Walensky RP, Chiosi JJ, Weinstein MC, Hicks PL, Aaronson WH, Moore RD, Paltiel AD, Freedberg KA. Racial and sex disparities in life expectancy losses among HIV-infected persons in the united states: impact of risk behavior, late initiation, and early discontinuation of antiretroviral therapy. Clin Infect Dis. 2009;49:1570–1578. - PMC - PubMed
-
- Justice AC, Freiberg MS, Tracy R, Tate J, Goetz M, Butt AA, Rodriguez-Barradas M, Gibert C, Oursler KA, Bryant KJ the VACS Project Team. Does an Index Composed of Clinical Data Reflect Effects of Inflammation, Coagulation, and Mnoocyte Activation on Mortality Among those Aging with HIV? Clinical Infectious Diseases. 2012 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UO1-AI-35004/AI/NIAID NIH HHS/United States
- T32 ES007069/ES/NIEHS NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- U01 DA036297/DA/NIDA NIH HHS/United States
- UO1-HD-32632/HD/NICHD NIH HHS/United States
- U01-AI38855/AI/NIAID NIH HHS/United States
- T32 ES07069/ES/NIEHS NIH HHS/United States
- CBR-86906/CAPMC/ CIHR/Canada
- U01 AI069434/AI/NIAID NIH HHS/United States
- R24-AI067039/AI/NIAID NIH HHS/United States
- K23 AG024896/AG/NIA NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- UO1-AI-34994/AI/NIAID NIH HHS/United States
- K01 AI071725/AI/NIAID NIH HHS/United States
- U24 AA022001/AA/NIAAA NIH HHS/United States
- R01-HL095136/HL/NHLBI NIH HHS/United States
- UO1-AI-34989/AI/NIAID NIH HHS/United States
- R01 MH054907/MH/NIMH NIH HHS/United States
- Z01 CP010176/ImNIH/Intramural NIH HHS/United States
- R01-AG029154/AG/NIA NIH HHS/United States
- AI-69432/AI/NIAID NIH HHS/United States
- TGF-96118/CAPMC/ CIHR/Canada
- U01 AI031834/AI/NIAID NIH HHS/United States
- HCP-97105/CAPMC/ CIHR/Canada
- K01-AI071754/AI/NIAID NIH HHS/United States
- U01-AI38858/AI/NIAID NIH HHS/United States
- UM1 AI069434/AI/NIAID NIH HHS/United States
- UO1-AI-35042/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- P30 AI054999/AI/NIAID NIH HHS/United States
- R01-DA04334/DA/NIDA NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- R01 HL090342/HL/NHLBI NIH HHS/United States
- R01 AG029154/AG/NIA NIH HHS/United States
- 5-MO1-RR-00052/RR/NCRR NIH HHS/United States
- R01 DA004334/DA/NIDA NIH HHS/United States
- UO1-AI-35040/AI/NIAID NIH HHS/United States
- U01-AI68636/AI/NIAID NIH HHS/United States
- AI-69434/AI/NIAID NIH HHS/United States
- U10-AA13566/AA/NIAAA NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01-AI68634/AI/NIAID NIH HHS/United States
- R01-MH54907/MH/NIMH NIH HHS/United States
- KRS-86251/CAPMC/ CIHR/Canada
- UO1-AI-35041/AI/NIAID NIH HHS/United States
- K23-AI-61-0320/AI/NIAID NIH HHS/United States
- CBR-94036/CAPMC/ CIHR/Canada
- U01 AI035041/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- R01-HL090342/HL/NHLBI NIH HHS/United States
- U01-AI069918/AI/NIAID NIH HHS/United States
- U01-AA013566/AA/NIAAA NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- ZIA CP010214/ImNIH/Intramural NIH HHS/United States
- K01 AI071754/AI/NIAID NIH HHS/United States
- P30-AI50410/AI/NIAID NIH HHS/United States
- UO1-AI-34993/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- U10 AA013566/AA/NIAAA NIH HHS/United States
- UL1-RR024131/RR/NCRR NIH HHS/United States
- R01-DA12568/DA/NIDA NIH HHS/United States
- U01 AI068636/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- P30-AI27757/AI/NIAID NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- R01 AG026250/AG/NIA NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- HL100347/HL/NHLBI NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- RR025747/RR/NCRR NIH HHS/United States
- U01 AA013566/AA/NIAAA NIH HHS/United States
- N02 CP055504/CP/NCI NIH HHS/United States
- U01 AI035043/AI/NIAID NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- UL1 RR025747/RR/NCRR NIH HHS/United States
- UO1-AI-35039/AI/NIAID NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- UO1-AI-42590/AI/NIAID NIH HHS/United States
- P30-AI27767/AI/NIAID NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- RC1 HL100347/HL/NHLBI NIH HHS/United States
- R01-DA11602/DA/NIDA NIH HHS/United States
- UO1-AI-31834/AI/NIAID NIH HHS/United States
- K01-AI071725/AI/NIAID NIH HHS/United States
- R01 HL095136/HL/NHLBI NIH HHS/United States
- 169621/CAPMC/ CIHR/Canada
- U01 AI035039/AI/NIAID NIH HHS/United States
- UO1-AI-35043/AI/NIAID NIH HHS/United States
- U01 AI068634/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
- P30-AI54999/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
