

Changing facial phenotype in Cohen syndrome: towards clues for an earlier diagnosis
- PMID: 23188044
- PMCID: PMC3722949
- DOI: 10.1038/ejhg.2012.251
Changing facial phenotype in Cohen syndrome: towards clues for an earlier diagnosis
Abstract
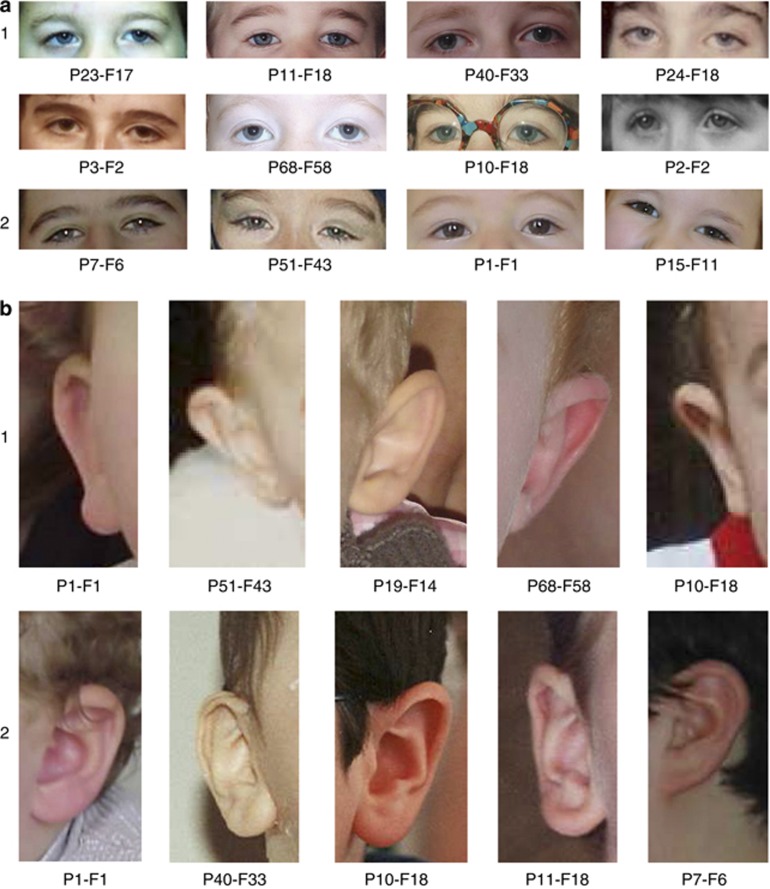
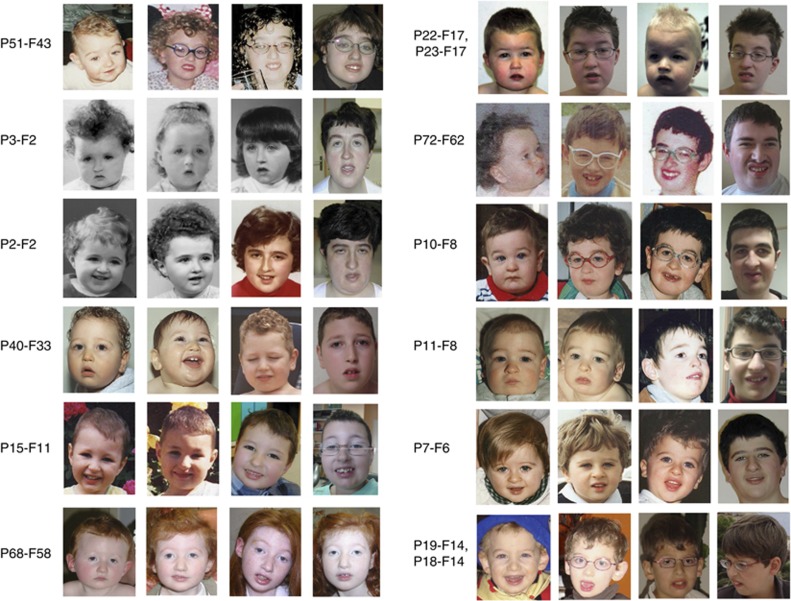
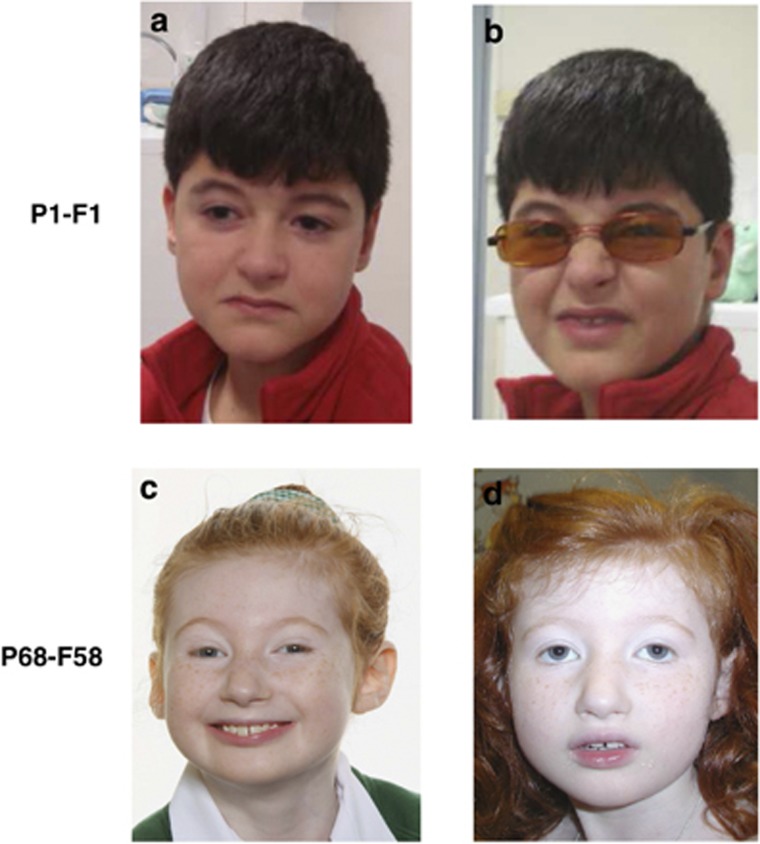
Cohen syndrome (CS) is a rare autosomal recessive condition caused by mutations and/or large rearrangements in the VPS13B gene. CS clinical features, including developmental delay, the typical facial gestalt, chorioretinal dystrophy (CRD) and neutropenia, are well described. CS diagnosis is generally raised after school age, when visual disturbances lead to CRD diagnosis and to VPS13B gene testing. This relatively late diagnosis precludes accurate genetic counselling. The aim of this study was to analyse the evolution of CS facial features in the early period of life, particularly before school age (6 years), to find clues for an earlier diagnosis. Photographs of 17 patients with molecularly confirmed CS were analysed, from birth to preschool age. By comparing their facial phenotype when growing, we show that there are no special facial characteristics before 1 year. However, between 2 and 6 years, CS children already share common facial features such as a short neck, a square face with micrognathia and full cheeks, a hypotonic facial appearance, epicanthic folds, long ears with an everted upper part of the auricle and/or a prominent lobe, a relatively short philtrum, a small and open mouth with downturned corners, a thick lower lip and abnormal eye shapes. These early transient facial features evolve to typical CS facial features with aging. These observations emphasize the importance of ophthalmological tests and neutrophil count in children in preschool age presenting with developmental delay, hypotonia and the facial features we described here, for an earlier CS diagnosis.
Figures



Similar articles
-
A novel homozygous nonsense mutation of VPS13B associated with previously unreported features of Cohen syndrome.Am J Med Genet A. 2020 Mar;182(3):570-575. doi: 10.1002/ajmg.a.61435. Epub 2019 Dec 11. Am J Med Genet A. 2020. PMID: 31825161
-
Homozygosity mapping and whole exome sequencing provide exact diagnosis of Cohen syndrome in a Saudi family.Brain Dev. 2020 Sep;42(8):587-593. doi: 10.1016/j.braindev.2020.04.010. Epub 2020 May 10. Brain Dev. 2020. PMID: 32402540
-
Ophthalmic features of retinitis pigmentosa in Cohen syndrome caused by pathogenic variants in the VPS13B gene.Acta Ophthalmol. 2020 May;98(3):e316-e321. doi: 10.1111/aos.14255. Epub 2019 Oct 3. Acta Ophthalmol. 2020. PMID: 31580008
-
A novel VPS13B mutation in Cohen syndrome: a case report and review of literature.BMC Med Genet. 2020 Jun 30;21(1):140. doi: 10.1186/s12881-020-01075-1. BMC Med Genet. 2020. PMID: 32605629 Free PMC article. Review.
-
Clinical variability of genetic isolates of Cohen syndrome.Clin Genet. 2011 Jun;79(6):501-6. doi: 10.1111/j.1399-0004.2011.01669.x. Epub 2011 Apr 7. Clin Genet. 2011. PMID: 21418059 Review.
Cited by
-
Not quite type 1 or type 2, what now? Review of monogenic, mitochondrial, and syndromic diabetes.Rev Endocr Metab Disord. 2018 Mar;19(1):35-52. doi: 10.1007/s11154-018-9446-3. Rev Endocr Metab Disord. 2018. PMID: 29777474 Review.
-
Impact of genetic test interpretation on a VPS13B missense variant in Cohen syndrome.Front Neurosci. 2024 Dec 11;18:1488133. doi: 10.3389/fnins.2024.1488133. eCollection 2024. Front Neurosci. 2024. PMID: 39723426 Free PMC article.
-
A prospective evaluation of whole-exome sequencing as a first-tier molecular test in infants with suspected monogenic disorders.Genet Med. 2016 Nov;18(11):1090-1096. doi: 10.1038/gim.2016.1. Epub 2016 Mar 3. Genet Med. 2016. PMID: 26938784
-
Novel VPS13B Mutations in Three Large Pakistani Cohen Syndrome Families Suggests a Baloch Variant with Autistic-Like Features.BMC Med Genet. 2015 Jun 25;16:41. doi: 10.1186/s12881-015-0183-0. BMC Med Genet. 2015. PMID: 26104215 Free PMC article.
-
Biallelic BICD2 variant is a novel candidate for Cohen-like syndrome.J Hum Genet. 2022 Sep;67(9):553-556. doi: 10.1038/s10038-022-01032-1. Epub 2022 Mar 25. J Hum Genet. 2022. PMID: 35338243 Free PMC article.
References
-
- Balikova I, Lehesjoki AE, de Ravel TJ, et al. Deletions in the VPS13B (COH1) Gene as a Cause of Cohen Syndrome. Hum Mutat. 2009;30:E845–E854. - PubMed
-
- Rivera-Brugués N, Albrecht B, Wieczorek D, et al. Cohen syndrome diagnosis using whole genome arrays. J Med Genet. 2011;48:136–140. - PubMed
-
- El Chehadeh-Djebbar S, Faivre L, Moncla A, et al. The power of high-resolution non-targeted array-CGH in identifying intragenic rearrangements responsible for Cohen syndrome. J Med Genet. 2011;48:e1. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
