

Mid-upper arm circumference based nutrition programming: evidence for a new approach in regions with high burden of acute malnutrition
- PMID: 23189140
- PMCID: PMC3506602
- DOI: 10.1371/journal.pone.0049320
Mid-upper arm circumference based nutrition programming: evidence for a new approach in regions with high burden of acute malnutrition
Abstract
Background: In therapeutic feeding programs (TFP), mid-upper arm circumference (MUAC) shows advantages over weight-for-height Z score (WHZ) and is recommended by the World Health Organization (WHO) as an independent criterion for screening children 6-59 months old. Here we report outcomes and treatment response from a TFP using MUAC ≤118 mm or oedema as sole admission criteria for severe acute malnutrition (SAM).
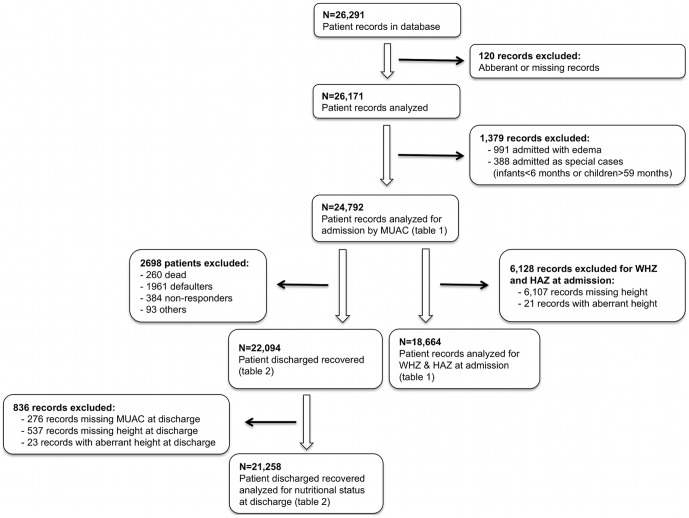
Methods: Patient data from September 2007 to March 2009 for children admitted by MUAC ≤118 mm or oedema to a Médecins Sans Frontières (MSF) TFP in Burkina Faso were retrospectively analyzed. Analysis included anthropometric measurements at admission and discharge, program outcomes and treatment response.
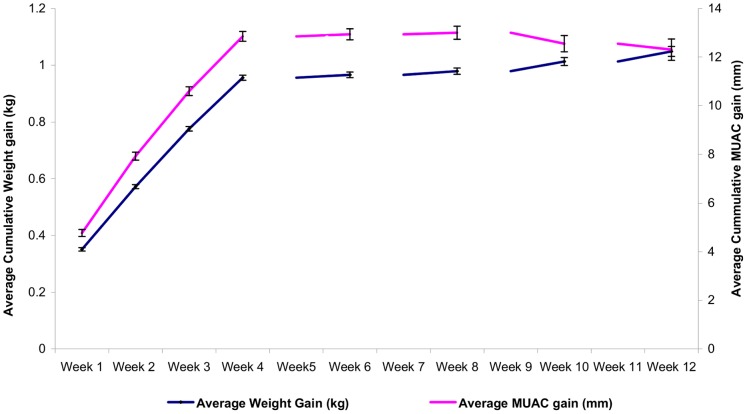
Results: Of 24,792 patient outcomes analyzed, nearly half (48.8%; n = 12,090) were admitted with MUAC 116-118 mm. Most patients (88.7%; n = 21,983) were 6-24 months old. At admission, 52.7% (n = 5,041) of those with MUAC 116-118 mm had a WHZ <-3 SD. At discharge, 89.1% (n = 22,094) recovered (15% weight gain or oedema resolution), 7.9% (n = 1,961) defaulted, 1.5% (n = 384) failed to respond to treatment, and 1.0% (n = 260) died. Average weight gain was 5.4 g/kg/day, and average MUAC gain was 0.42 mm/day. Patients with MUAC ≤114 mm at admission had higher average daily weight and MUAC gains at discharge compared to those admitted with MUAC 116-118 mm, but those in the latter category required longer lengths of stay to achieve recovery (P<0.001).
Conclusion: This analysis suggests that MUAC ≤118 mm as TFP admission criterion is a useful alternative to WHZ. Regarding treatment response, rates of weight and MUAC gain were acceptable. Applying 15% weight gain as discharge criterion resulted in longer lengths of stay for less malnourished children. Since MUAC gain parallels weight gain, it may be feasible to use MUAC as both an admission and discharge criterion.
Conflict of interest statement
Figures
References
-
- Caulfield LE, de Onis M, Blössner M, Black RE (2004) Undernutrition as an underlying cause of child deaths associated with diarrhea, pneumonia, malaria, and measles. Am J Clin Nutr 80: 193–198. - PubMed
-
- Collins S, Sadler K (2002) Outpatient care for severely malnourished children in emergency relief programmes: a retrospective cohort study. Lancet 360: 1824–1830. - PubMed
-
- WHO/UNICEF/WFP/SCN Joint Statement (2007) Community-based management of severe acute malnutrition. Available: http://www.who.int/child_adolescent_health/documents/pdfs/severe_acute_m.... Accessed 2012 Feb 29.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
