

Antiretroviral agents and prevention of malaria in HIV-infected Ugandan children
- PMID: 23190222
- PMCID: PMC3664297
- DOI: 10.1056/NEJMoa1200501
Antiretroviral agents and prevention of malaria in HIV-infected Ugandan children
Abstract
Background: Human immunodeficiency virus (HIV) protease inhibitors show activity against Plasmodium falciparum in vitro. We hypothesized that the incidence of malaria in HIV-infected children would be lower among children receiving lopinavir-ritonavir-based antiretroviral therapy (ART) than among those receiving nonnucleoside reverse-transcriptase inhibitor (NNRTI)-based ART.
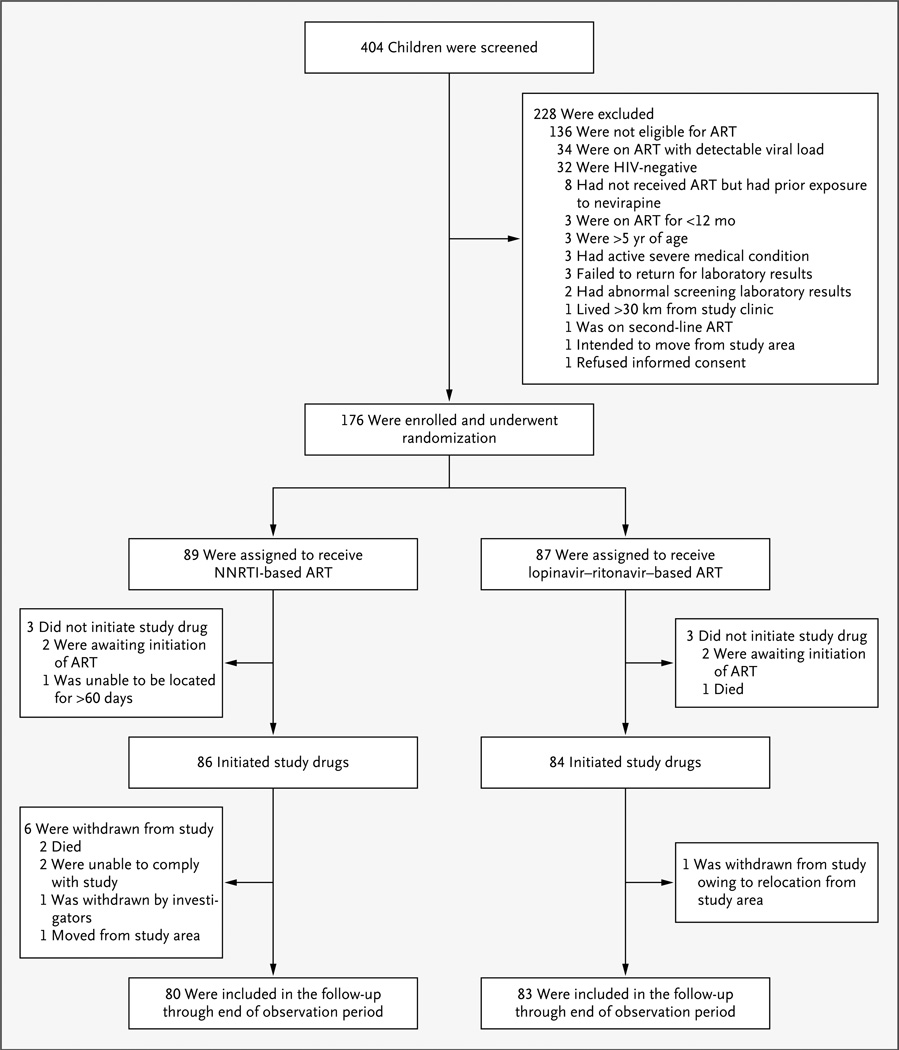
Methods: We conducted an open-label trial in which HIV-infected children 2 months to 5 years of age who were eligible for ART or were currently receiving NNRTI-based ART were randomly assigned to either lopinavir-ritonavir-based ART or NNRTI-based ART and were followed for 6 months to 2 years. Cases of uncomplicated malaria were treated with artemether-lumefantrine. The primary end point was the incidence of malaria.
Results: We enrolled 176 children, of whom 170 received the study regimen: 86 received NNRTI-based ART, and 84 lopinavir-ritonavir-based ART. The incidence of malaria was lower among children receiving the lopinavir-ritonavir-based regimen than among those receiving the NNRTI-based regimen (1.32 vs. 2.25 episodes per person-year; incidence-rate ratio, 0.59; 95% confidence interval [CI], 0.36 to 0.97; P=0.04), as was the risk of a recurrence of malaria after treatment with artemether-lumefantrine (28.1% vs. 54.2%; hazard ratio, 0.41; 95% CI, 0.22 to 0.76; P=0.004). The median lumefantrine level on day 7 after treatment for malaria was significantly higher in the lopinavir-ritonavir group than in the NNRTI group. In the lopinavir-ritonavir group, lumefantrine levels exceeding 300 ng per milliliter on day 7 were associated with a reduction of more than 85% in the 63-day risk of recurrent malaria. A greater number of serious adverse events occurred in the lopinavir-ritonavir group than in the NNRTI group (5.6% vs. 2.3%, P=0.16). Pruritus occurred significantly more frequently in the lopinavir-ritonavir group, and elevated alanine aminotransferase levels significantly more frequently in the NNRTI group.
Conclusions: Lopinavir-ritonavir-based ART as compared with NNRTI-based ART reduced the incidence of malaria by 41%, with the lower incidence attributable largely to a significant reduction in the recurrence of malaria after treatment with artemether-lumefantrine. Lopinavir-ritonavir-based ART was accompanied by an increase in serious adverse events. (Funded by the Eunice Kennedy Shriver National Institute of Child Health and Human Development; ClinicalTrials.gov number, NCT00978068.).
Figures


References
-
- Kamya MR, Gasasira AF, Achan J, et al. Effects of trimethoprim-sulfamethoxazole and insecticide-treated bednets on malaria among HIV-infected Ugandan children. AIDS. 2007;21:2059–2066. - PubMed
-
- Skinner-Adams TS, McCarthy JS, Gardiner DL, Hilton PM, Andrews KT. Antiretrovirals as antimalarial agents. J Infect Dis. 2004;190:1998–2000. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical