

Elevated troponin I and its prognostic significance in acute liver failure
- PMID: 23190744
- PMCID: PMC3672613
- DOI: 10.1186/cc11883
Elevated troponin I and its prognostic significance in acute liver failure
Abstract
Introduction: Acute liver failure (ALF) is a life-threatening multisystem illness complicated by multiple organ failure (MOF) and haemodynamic disturbances. Morbidity and mortality remains high and various prognostic and scoring models are in use to predict outcome. A recent observation in a large cohort of ALF patients suggested a prognostic value of troponin I (cTnI) and its role as a marker of subclinical myocardial injury and outcome.
Methods: Data from consecutive ALF patients over a four-year period from January 2007 to March 2011 were included. The aim of this study was to correlate any relationship that may exist between cTnI, mortality, severity of illness and non-hepatic organ failure.
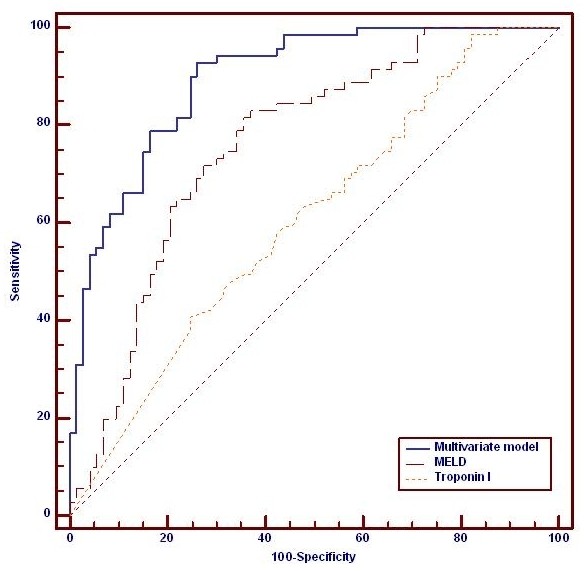
Results: A total of 218 subjects (age 36 (16 to 90) years, M:F 103:115) were studied, of which 136 had an elevated cTnI > 0.05 μg/L. Higher organ failure scores were found with positive cTnI: APACHE II (19.5 (3 to 51) vs 14 (2 to 51), P = 0.001), APACHE III (81 (15 to 148) vs 59 (8 to 172), P = < 0.001) SOFA (15 (4 to 20) vs 13 (2 to 21), P = 0.027) and SAPS (48 (12 to 96) vs 34 (12 to 97), P = 0.001). Patients with positive cTnI had higher serum creatinine (192 μmol/l (38 to 550) vs 117 μmol/l (46 to 929), P < 0.001), arterial lactate (0.25, P < 0.001) and a lower pH (-0.21, P = 0.002). Also a higher proportion required renal replacement therapy (78% vs 60%, P = 0.006). Patients with elevated cTnI more frequently required vasopressors-norepinephrine (73% vs 50%, P = 0.008). Elevated cTnI did not predict outcome as effectively as other models (AUROC 0.61 (95% CI 0.52 to 0.68)).
Conclusions: More than 60% of ALF patients in this study demonstrated elevated cTnI. Despite a close correlation with organ failure severity, cTnI was a poor independent predictor of outcome. cTnI may not represent true myocardial injury and may be better viewed as a marker of metabolic stress.
Figures
Comment in
-
Acute liver failure and elevated troponin-I: controversial results and significance?Crit Care. 2013 Jan 14;17(1):102. doi: 10.1186/cc11897. Crit Care. 2013. PMID: 23316924 Free PMC article.
References
-
- Trey C, Lipworth L, Davidson CS. Halothane and liver damage. N Engl J Med. 1969;16:562–563. - PubMed
-
- Lee WM. Acute liver failure in the United States. Semin Liver Dis. 2003;16:217–226. - PubMed
-
- Rolando N, Wade J, Davalos M, Wendon J, Philpott-Howard J, Williams R. The systemic inflammatory response syndrome in acute liver failure. Hepatology. 2000;16:734–739. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
