

Comprehensive self management and routine monitoring in chronic obstructive pulmonary disease patients in general practice: randomised controlled trial
- PMID: 23190905
- PMCID: PMC3514071
- DOI: 10.1136/bmj.e7642
Comprehensive self management and routine monitoring in chronic obstructive pulmonary disease patients in general practice: randomised controlled trial
Abstract
Objective: To assess the long term effects of two different modes of disease management (comprehensive self management and routine monitoring) on quality of life (primary objective), frequency and patients' management of exacerbations, and self efficacy (secondary objectives) in patients with chronic obstructive pulmonary disease (COPD) in general practice.
Design: 24 month, multicentre, investigator blinded, three arm, pragmatic, randomised controlled trial.
Setting: 15 general practices in the eastern part of the Netherlands.
Participants: Patients with COPD confirmed by spirometry and treated in general practice. Patients with very severe COPD or treated by a respiratory physician were excluded.
Interventions: A comprehensive self management programme as an adjunct to usual care, consisting of four tailored sessions with ongoing telephone support by a practice nurse; routine monitoring as an adjunct to usual care, consisting of 2-4 structured consultations a year with a practice nurse; or usual care alone (contacts with the general practitioner at the patients' own initiative).
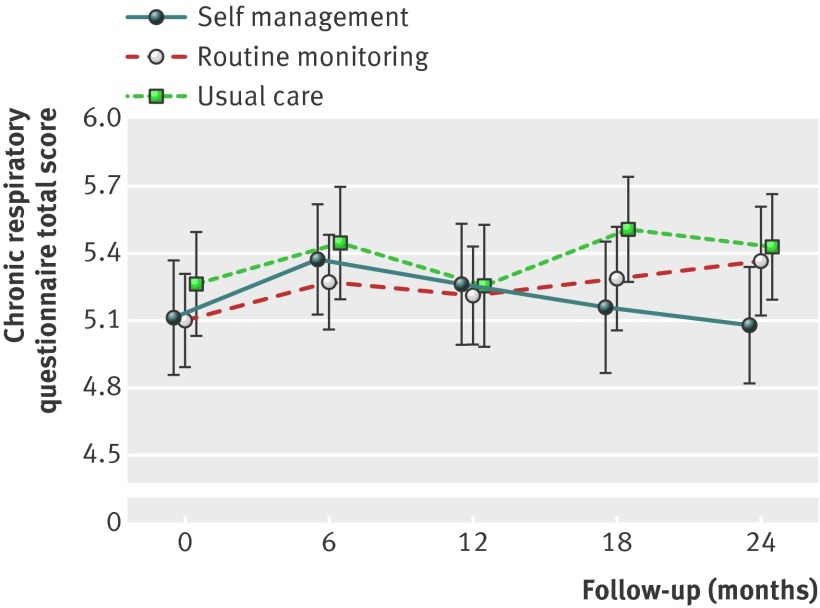
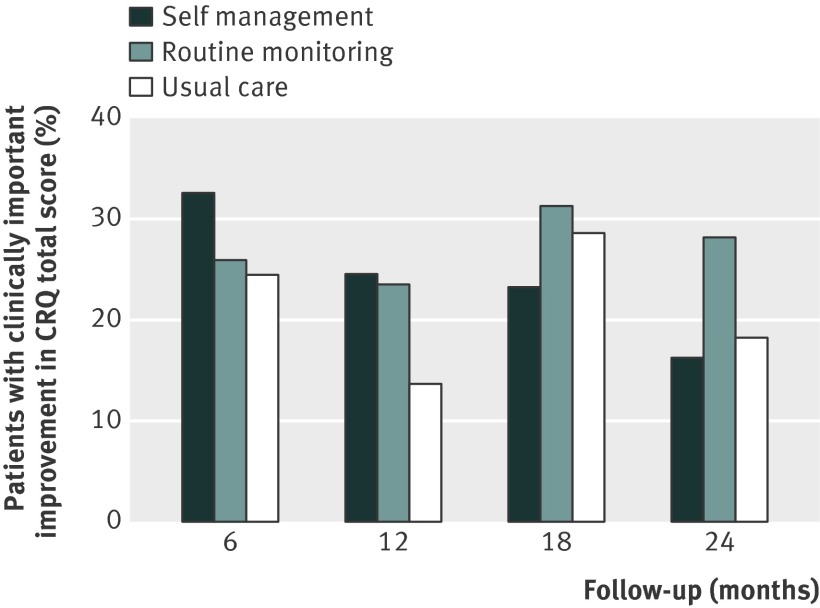
Outcome measures: The primary outcome was the change in COPD specific quality of life at 24 months as measured with the chronic respiratory questionnaire total score. Secondary outcomes were chronic respiratory questionnaire domain scores, frequency and patients' management of exacerbations measured with the Nijmegen telephonic exacerbation assessment system, and self efficacy measured with the COPD self-efficacy scale.
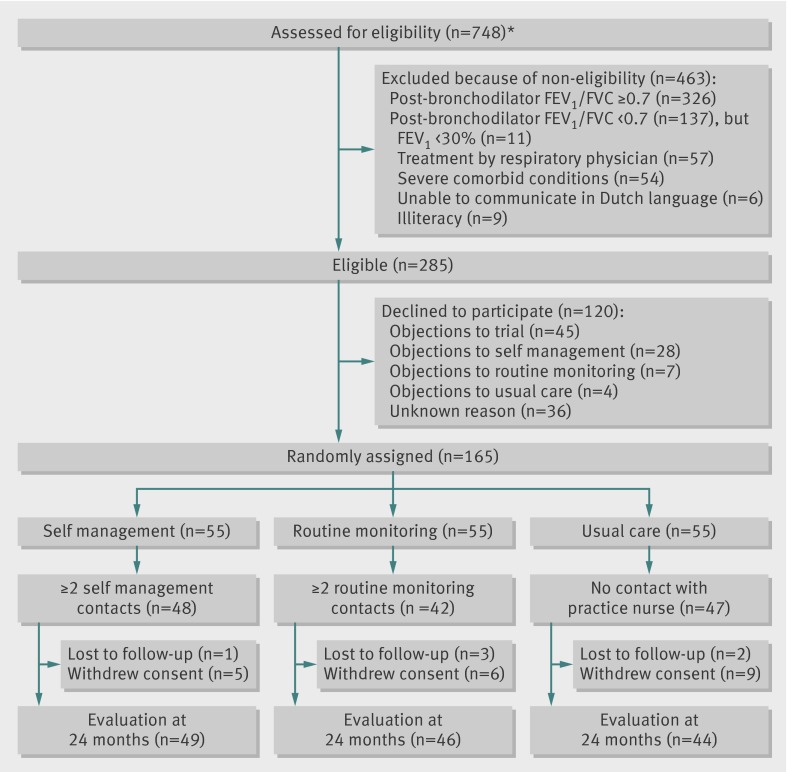
Results: 165 patients were allocated to self management (n=55), routine monitoring (n=55), or usual care alone (n=55). At 24 months, adjusted treatment differences between the three groups in mean chronic respiratory questionnaire total score were not significant. Secondary outcomes did not differ, except for exacerbation management. Compared with usual care, more exacerbations in the self management group were managed with bronchodilators (odds ratio 2.81, 95% confidence interval 1.16 to 6.82) and with prednisolone, antibiotics, or both (3.98, 1.10 to 15.58).
Conclusions: Comprehensive self management or routine monitoring did not show long term benefits in terms of quality of life or self efficacy over usual care alone in COPD patients in general practice. Patients in the self management group seemed to be more capable of appropriately managing exacerbations than did those in the usual care group.
Trial registration: Clinical trials NCT00128765.
Conflict of interest statement
Competing interests: All authors have completed the Unified Competing Interest form at
Figures
References
-
- Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: revised 2011. GOLD, 2011 (available from www.goldcopd.org).
-
- Van den Bemt L, Schermer T, Smeele I, Bischoff E, Jacobs A, Grol R, et al. Monitoring of patients with COPD: a review of current guidelines’ recommendations. Respir Med 2008;102:633-41. - PubMed
-
- Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management of chronic disease in primary care. JAMA 2002;288:2469-75. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical