

Multiple Acetabular Revisions in THA - Poor Outcome Despite Maximum Effort
- PMID: 23193432
- PMCID: PMC3504796
- DOI: 10.2174/1874325001206010488
Multiple Acetabular Revisions in THA - Poor Outcome Despite Maximum Effort
Erratum in
- Open Orthop J. 2012 Dec 12;6:588. Seeger, Jb [corrected to Seeger, J B]; Krüge, M [corrected to Krüger, M]; Bitsch, Bg [corrected to Bitsch, R G]
Abstract
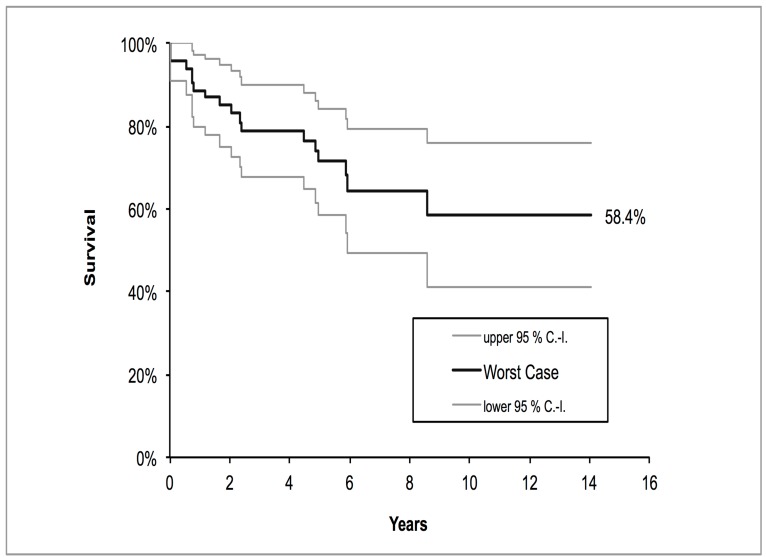
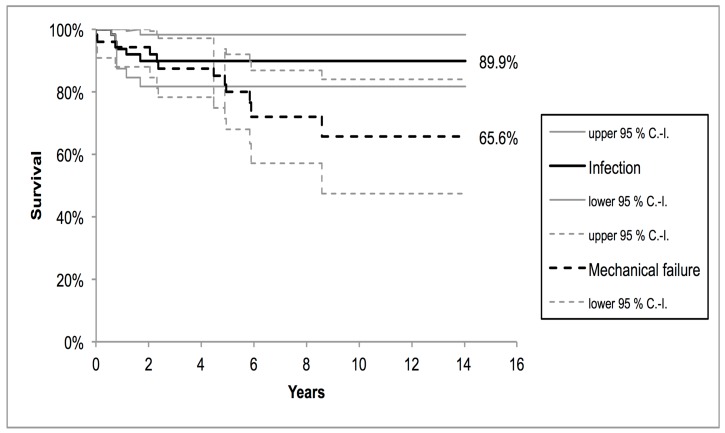
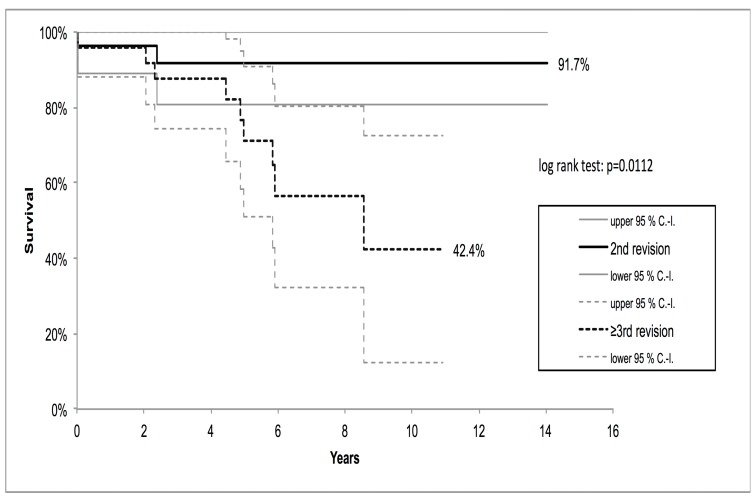
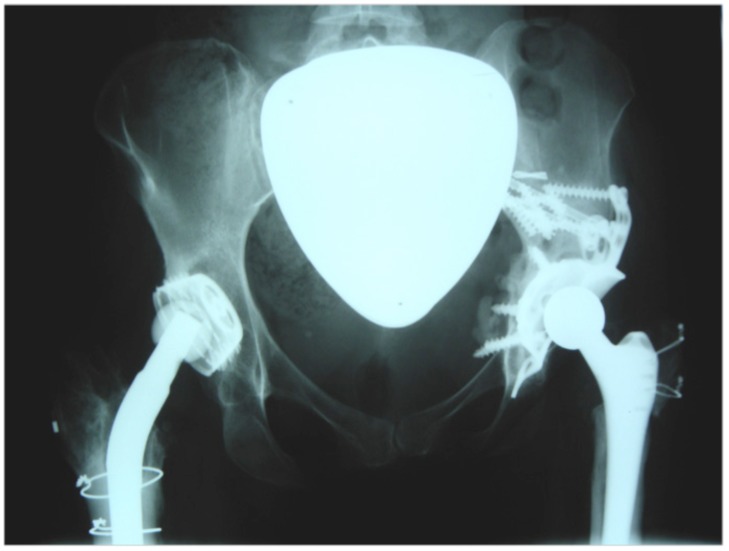
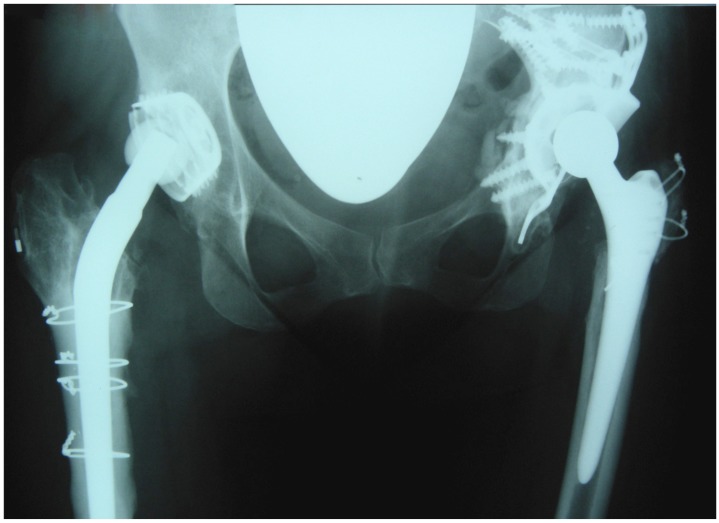
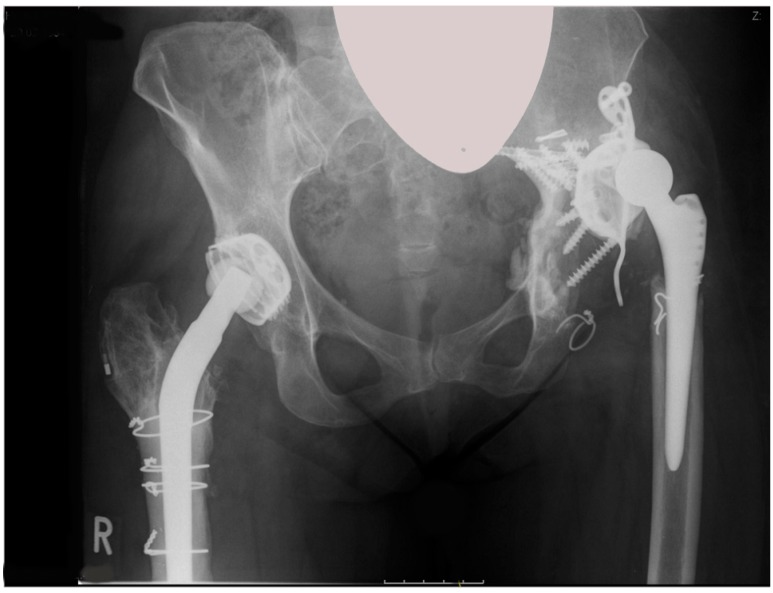
A consecutive series of 52 acetabular revisions was evaluated retrospectively. Inclusion criteria for all patients were at least one former exchange of the acetabular component. Reconstruction was performed with reliable techniques and implants other than extensively porous coated device (e.g. tantalum). The mean follow up was 5.63 (0.01-14.05) years. Cumulative survival at 14.05 years with removal of the acetabular component due to aseptic loosening or the worst case criterion (removal of the acetabular component for any cause and/or lost to follow-up) as the end point was 66.38 (95 % C.-I.: 47.80-84.96) % and 58.42 (95 % C.-I.: 41.01-75.83) %, respectively. The cumulative survival rate with mechanical failure of the acetabular reconstruction as the endpoint was significantly lower in patients with two or more previous revisions in comparison to those with only one former procedure (log rank test: p=0,0112 respectively). The mean Merle d'Aubignée-score improved from 7.3 (0-14) preoperatively to 10.6 (0-17) points at latest follow up examination.Survival of acetabular reconstructions with common techniques and implants is decreasing with the number of previous revisions. This may cause major concerns with regard to the rising number of patients needing repeated revisions. Maximizing durability of primary THA, precise preoperative planning as well as improved techniques and implants for revision may decrease this problem in the long term.
Keywords: Hip arthroplasty; acetabular reconstruction.; porous metal device; revision; tantalum.
Figures

References
-
- Kurtz S, Ong K, Lau E, Mowat F, Halpern M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J Bone Joint Surg Am. 2007;89(4):780–5. - PubMed
-
- Pedersen AB, Johnsen SP, Overgaard S, Søballe K, Sørensen HT, Lucht U. Total hip arthroplasty in Denmark: incidence of primary operations and revisions during 1996-2002 and estimated future demands. Acta Orthop. 2005;76(2):182–9. - PubMed
-
- Schlegel UJ, Bitsch RG, Pritsch M, Clauss M, Mau H, Breusch SJ. Mueller reinforcement rings in acetabular revision: outcome in 164 hips followed for 2-17 years. Acta Orthop. 2006;77(2):234–41. - PubMed
-
- Regis D, Magnan B, Sandri A, Bartolozzi P. Long-term results of anti-protrusion cage and massive allografts for the management of periprosthetic acetabular bone loss. J Arthroplasty. 2008;23(6):826–32. - PubMed
LinkOut - more resources
Full Text Sources