

Myasthenia gravis: a review
- PMID: 23193443
- PMCID: PMC3501798
- DOI: 10.1155/2012/874680
Myasthenia gravis: a review
Abstract
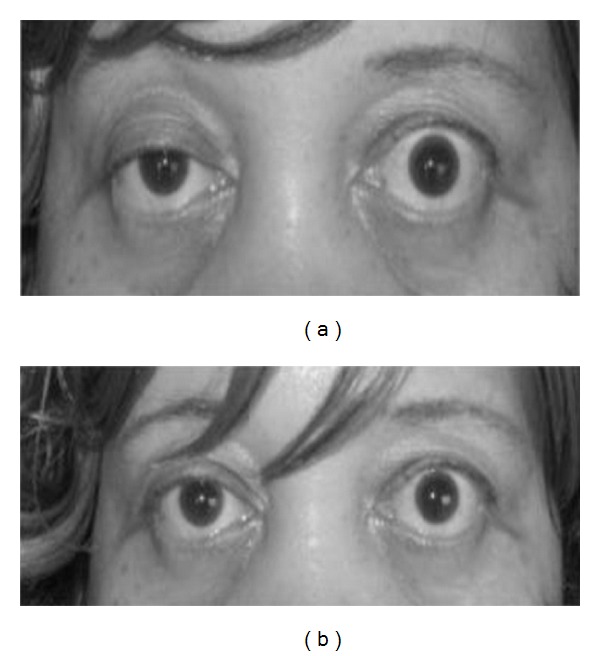
Acquired myasthenia gravis is a relatively uncommon disorder, with prevalence rates that have increased to about 20 per 100,000 in the US population. This autoimmune disease is characterized by muscle weakness that fluctuates, worsening with exertion, and improving with rest. In about two-thirds of the patients, the involvement of extrinsic ocular muscle presents as the initial symptom, usually progressing to involve other bulbar muscles and limb musculature, resulting in generalized myasthenia gravis. Although the cause of the disorder is unknown, the role of circulating antibodies directed against the nicotinic acetylcholine receptor in its pathogenesis is well established. As this disorder is highly treatable, prompt recognition is crucial. During the past decade, significant progress has been made in our understanding of the disease, leading to new treatment modalities and a significant reduction in morbidity and mortality.
Figures
Similar articles
-
Myasthenia gravis.Dis Mon. 1997 Feb;43(2):65-109. doi: 10.1016/s0011-5029(97)90033-x. Dis Mon. 1997. PMID: 9118787 Review.
-
[Myasthenia gravis].Internist (Berl). 2016 Apr;57(4):349-61. doi: 10.1007/s00108-016-0035-9. Internist (Berl). 2016. PMID: 27000188 German.
-
Pearls: myasthenia.Semin Neurol. 2010 Feb;30(1):35-7. doi: 10.1055/s-0029-1244999. Epub 2010 Feb 1. Semin Neurol. 2010. PMID: 20127579
-
Eye muscle antibodies in patients with ocular myasthenia gravis: possible mechanism for eye muscle inflammation in acetylcholine-receptor antibody-negative patients.Clin Immunol Immunopathol. 1998 Jun;87(3):276-81. doi: 10.1006/clin.1998.4536. Clin Immunol Immunopathol. 1998. PMID: 9646837
-
Myasthenia Gravis and Congenital Myasthenic Syndromes.Continuum (Minneap Minn). 2019 Dec;25(6):1767-1784. doi: 10.1212/CON.0000000000000800. Continuum (Minneap Minn). 2019. PMID: 31794470 Review.
Cited by
-
IL-6 receptor antibody treatment improves muscle weakness in experimental autoimmune myasthenia gravis mouse model.Front Neurol. 2024 May 1;15:1356300. doi: 10.3389/fneur.2024.1356300. eCollection 2024. Front Neurol. 2024. PMID: 38751878 Free PMC article.
-
Conservation and Innovation: Versatile Roles for LRP4 in Nervous System Development.J Dev Biol. 2021 Mar 14;9(1):9. doi: 10.3390/jdb9010009. J Dev Biol. 2021. PMID: 33799485 Free PMC article. Review.
-
Exploring the Gut Microbiome in Myasthenia Gravis.Nutrients. 2022 Apr 14;14(8):1647. doi: 10.3390/nu14081647. Nutrients. 2022. PMID: 35458209 Free PMC article. Review.
-
Abnormalities of Otoacoustic Emissions in Myasthenia Gravis: Association With Serological and Electrophysiological Features.Front Neurol. 2018 Dec 20;9:1124. doi: 10.3389/fneur.2018.01124. eCollection 2018. Front Neurol. 2018. PMID: 30619074 Free PMC article.
-
D-penicillamine Induced Myasthenia Gravis in Wilson's Disease: A Case Report.JNMA J Nepal Med Assoc. 2022 Jul 1;60(251):644-647. doi: 10.31729/jnma.7607. JNMA J Nepal Med Assoc. 2022. PMID: 36705187 Free PMC article.
References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
