

Racial disparities in surgical resection and survival among elderly patients with poor prognosis cancer
- PMID: 23195204
- PMCID: PMC4547837
- DOI: 10.1016/j.jamcollsurg.2012.09.019
Racial disparities in surgical resection and survival among elderly patients with poor prognosis cancer
Abstract
Background: Reports indicate that black patients have lower survival after the diagnosis of a poor prognosis cancer, compared with white patients. We explored the extent to which this disparity is attributable to the underuse of surgery.
Study design: Using the Surveillance, Epidemiology, and End Results program and Medicare database, we identified 57,364 patients, ages 65 years and older, with a new diagnosis of nonmetastatic liver, lung, pancreatic, and esophageal cancer, from 2000 to 2005. We evaluated racial differences in resection rates after adjustment for patient, tumor, and hospital characteristics using hierarchical logistic regression. Cox proportional hazards regression was used to assess racial differences in survival after adjusting for patient, tumor, and hospital characteristics, and receipt of surgery.
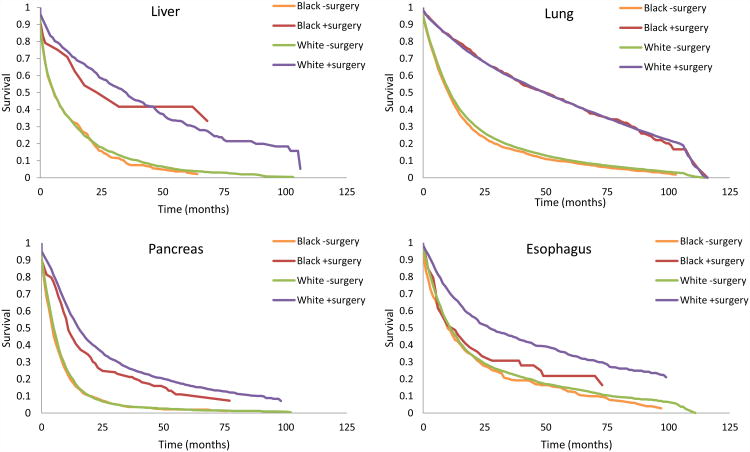
Results: Compared with white patients, black patients were less likely to undergo surgery for liver (adjusted odds ratio [aOR] = 0.49; 95% CI, 0.29-0.83), lung (aOR = 0.62; 95% CI, 0.56-0.69), pancreas (aOR = 0.53; 95% CI, 0.41-0.70), and esophagus cancers (aOR = 0.64; 95% CI, 0.42-0.99). Hospitals varied in their surgery rates among patients with potentially resectable disease. However, resection rates were consistently lower for black patients, regardless of the resection rate of the treating hospital. Although there were no racial differences in overall survival with liver and esophageal cancer, black patients experienced poorer survival for lung (adjusted hazard ratio = 1.05; 95% CI, 1.00-1.10) and pancreas cancer (adjusted hazard ratio = 1.15; 95% CI, 1.03-1.30). In both instances, there were no residual racial disparities in overall survival after adjusting for use of surgery.
Conclusions: Black patients are less likely to undergo surgery after diagnosis of a poor prognosis cancer. Our findings suggest that surgery is an important predictor of overall mortality, and that efforts to reduce racial disparities will require stakeholders to gain a better understanding of why elderly black patients are less likely to get to the operating room.
Copyright © 2013 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Cancer of the Esophagus: 5-Year Relative and Period Survival (Percent) by Race, Sex, Diagnosis Year, Stage and Age. Surveillance, Epidemiology, and End Results (SEER) Program. Available from: http://seer.cancer.gov/csr/1975_2008/results_single/sect_08_table.08.pdf.
-
- Siegel R, Ward E, Brawley O, Jemal A. Cancer statistics, 2011: the impact of eliminating socioeconomic and racial disparities on premature cancer deaths. CA Cancer J Clin. 2011 Jul-Aug;61(4):212–236. - PubMed
-
- Bach PB, Cramer LD, Warren JL, Begg CB. Racial differences in the treatment of early-stage lung cancer. N Engl J Med. 1999 Oct 14;341(16):1198–1205. - PubMed
-
- Bach PB, Schrag D, Brawley OW, Galaznik A, Yakren S, Begg CB. Survival of blacks and whites after a cancer diagnosis. JAMA. 2002 Apr 24;287(16):2106–2113. - PubMed
-
- Murphy MM, Simons JP, Hill JS, et al. Pancreatic resection: a key component to reducing racial disparities in pancreatic adenocarcinoma. Cancer. 2009 Sep 1;115(17):3979–3990. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
