

Effects of radiotherapy on uveal melanomas and adjacent tissues
- PMID: 23196647
- PMCID: PMC3574249
- DOI: 10.1038/eye.2012.249
Effects of radiotherapy on uveal melanomas and adjacent tissues
Abstract
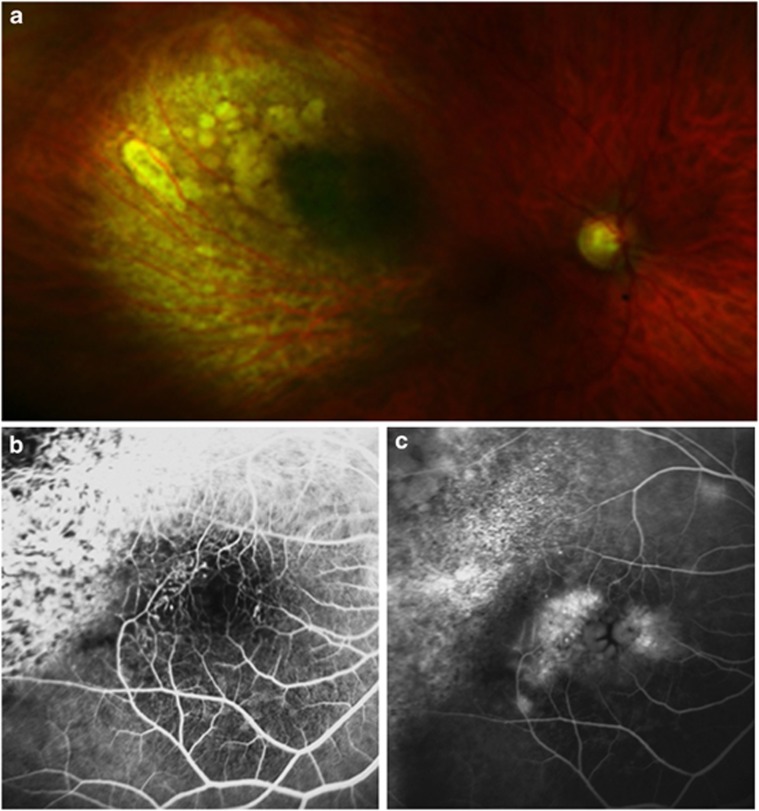
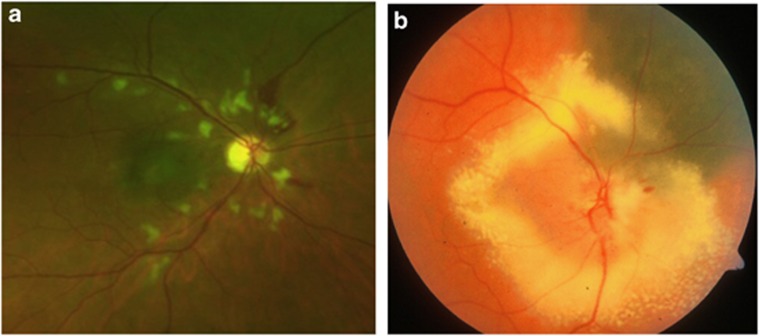
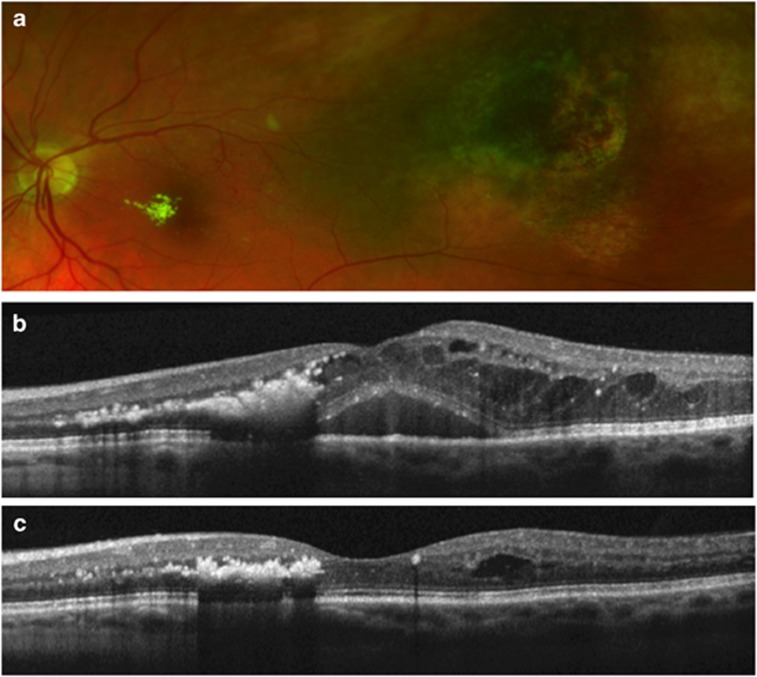
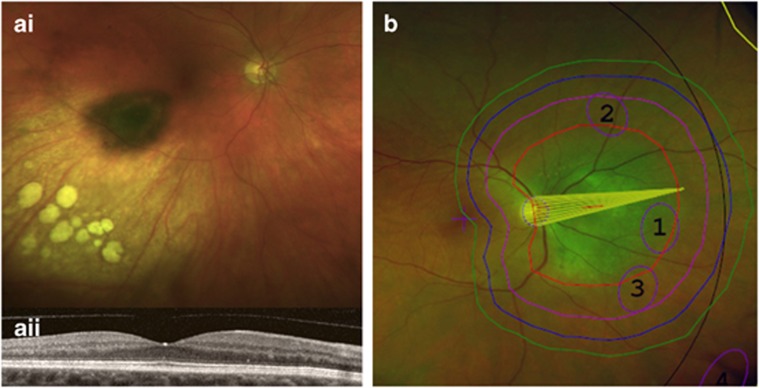
Most uveal melanomas are treated with radiotherapy. An adequate understanding of the effects of radiation on the tumour and the healthy ocular tissues is necessary. Ionizing radiation damages cell membranes, organelles, and DNA. Irradiated cells are lysed or undergo apoptosis, necrosis, and senescence. These effects occur in tumour cells and vascular endothelial cells, resulting in tumour shrinkage, ischaemia, infarction, exudation, and fibrosis, which can cause exudative maculopathy, serous retinal detachment, rubeosis, and neovascular glaucoma (ie, 'toxic tumour syndrome'). Such abnormalities must be distinguished from collateral damage to healthy ocular tissues that receive high doses of radiation, and these include radiation-induced retinopathy, optic neuropathy, choroidopathy, cataract, and scleral necrosis. Radiation retinopathy can be treated effectively with photodynamic therapy, anti-angiogenic agents, and intravitreal steroid injections. In some patients, optic neuropathy may improve with intravitreal steroids or anti-angiogenic agents. Neovascular glaucoma resolves with intra-cameral bevacizumab. Exudative retinal detachment can regress with intra-vitreal steroid injections. Cataract is treated in the usual manner. Scleral necrosis, if severe, may require grafting, possibly using a lamellar flap from the same eye. Depending on the bulk of the residual toxic tumour, treatment can consist of intra-vitreal steroids and/or anti-angiogenic agents, transpupillary thermotherapy or photodynamic therapy to the tumour, or surgical removal of the tumour by endo- or exo-resection. Measures aimed at preventing collateral damage include eccentric placement of ruthenium plaques or iodine seeds and delivery of a notched proton beam. The decision to treat a uveal melanoma with radiotherapy requires the ability to manage iatrogenic side effects and complications.
Figures
References
-
- Avery RB, Diener-West M, Reynolds SM, Grossniklaus HE, Green WR, Albert DM. Histopathologic characteristics of choroidal melanoma in eyes enucleated after iodine 125 brachytherapy in the collaborative ocular melanoma study. Arch Ophthalmol. 2008;126 (2:207–212. - PubMed
-
- Archer DB, Gardiner TA. Ionizing radiation and the retina. Curr Opin Ophthalmol. 1994;5 (3:59–65. - PubMed
-
- Amoaku WM, Lafaut B, Sallet G, De Laey JJ. Radiation choroidal vasculopathy: an indocyanine green angiography study. Eye (London, England) 1995;9 (Part 6:738–744. - PubMed
-
- Danesh-Meyer HV. Radiation-induced optic neuropathy. J Clin Neurosci. 2008;15 (2:95–100. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
