

Flash mob research: a single-day, multicenter, resident-directed study of respiratory rate
- PMID: 23197319
- PMCID: PMC3747725
- DOI: 10.1378/chest.12-1837
Flash mob research: a single-day, multicenter, resident-directed study of respiratory rate
Abstract
Background: Vital signs are critical data in the care of hospitalized patients, but the accuracy with which respiratory rates are recorded in this population remains uncertain. We used a novel flash mob research approach to evaluate the accuracy of recorded respiratory rates in inpatients.
Methods: This was a single-day, resident-led, prospective observational study of recorded vs directly observed vital signs in nonventilated patients not in the ICU on internal medicine teaching services at six large tertiary-care centers across the United States.
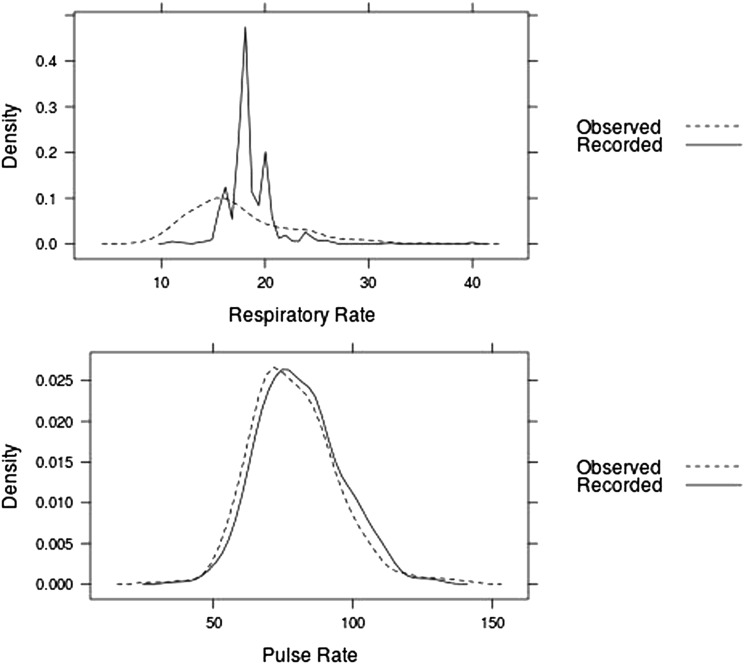
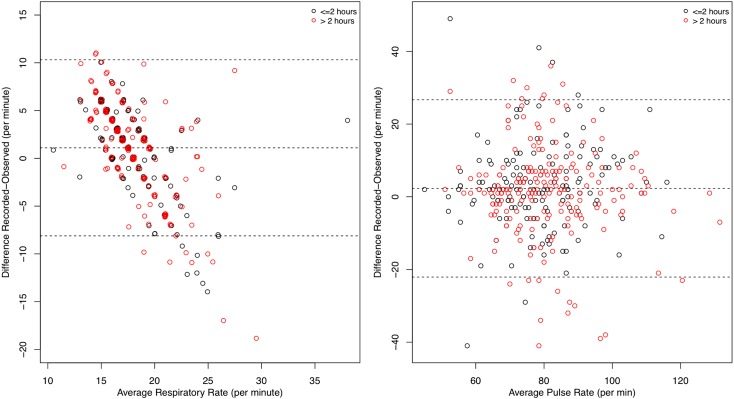
Results: Among the 368 inpatients included, the median respiratory rate was 16 breaths/min for the directly observed values and 18 breaths/min for the recorded values, with a median difference of 2 breaths/min (P < .001). Respiratory rates of 18 or 20 breaths/min accounted for 71.8% (95% CI, 67.1%-76.4%) of the recorded values compared with 13.0% (95% CI, 9.5%-16.5%) of the directly observed measurements. For individual patients, there was less agreement between the recorded and the directly observed respiratory rate compared with pulse rate.
Conclusions: Among hospitalized patients across the United States, recorded respiratory rates are higher than directly observed measurements and are significantly more likely to be 18 or 20 breaths/min.
Figures
References
-
- Jones AE, Yiannibas V, Johnson C, Kline JA. Emergency department hypotension predicts sudden unexpected in-hospital mortality: a prospective cohort study. Chest. 2006;130(4):941-946 - PubMed
-
- Ludikhuize J, Smorenburg SM, de Rooij SE, de Jonge E. Identification of deteriorating patients on general wards; measurement of vital parameters and potential effectiveness of the Modified Early Warning Score. J Crit Care. 2012;27(4):424–e7-424.e13.. - PubMed
-
- McBride J, Knight D, Piper J, Smith GB. Long-term effect of introducing an early warning score on respiratory rate charting on general wards. Resuscitation. 2005;65(1):41-44 - PubMed
-
- Fieselmann JF, Hendryx MS, Helms CM, Wakefield DS. Respiratory rate predicts cardiopulmonary arrest for internal medicine inpatients. J Gen Intern Med. 1993;8(7):354-360 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
