

Nutritional support teams increase percutaneous endoscopic gastrostomy uptake in motor neuron disease
- PMID: 23197892
- PMCID: PMC3508641
- DOI: 10.3748/wjg.v18.i44.6461
Nutritional support teams increase percutaneous endoscopic gastrostomy uptake in motor neuron disease
Abstract
Aim: To examine factors influencing percutaneous endoscopic gastrostomy (PEG) uptake and outcomes in motor neuron disease (MND) in a tertiary care centre.
Methods: Case notes from all patients with a confirmed diagnosis of MND who had attended the clinic at the Repatriation General Hospital between January 2007 and January 2011 and who had since died, were audited. Data were extracted for demographics (age and gender), disease characteristics (date of onset, bulbar or peripheral predominance, complications), date and nature of discussion of gastrostomy insertion, nutritional status [weight measurements, body mass index (BMI)], date of gastrostomy insertion and subsequent progress (duration of survival) and quality of life (QoL) [Amyotrophic Lateral Sclerosis Functional Rating Scale-Revised (ALSFRS-R)]. In addition, the type of clinician initiating the discussion regarding gastrostomy was recorded as Nutritional Support Team (involved in providing nutrition input viz Gastroenterologist, Speech Pathologist, Dietitian) and other (involved in non-nutritional aspects of patient care). Factors affecting placement and outcomes including length of survival, change in weight and QoL were determined.
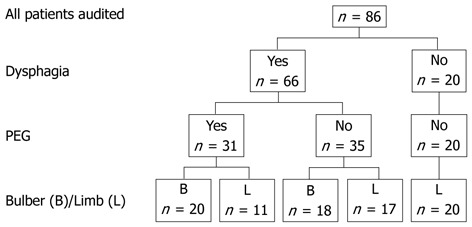
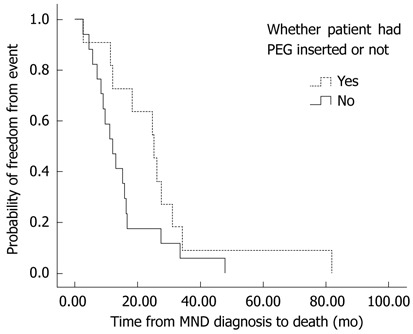
Results: Case records were available for all 86 patients (49 men, mean age at diagnosis 66.4 years). Thirty-eight patients had bulbar symptoms and 48 had peripheral disease as their presenting feature. Sixty-six patients reported dysphagia. Thirty-one patients had undergone gastrostomy insertion. The major indications for PEG placement were dysphagia and weight loss. Nine patients required immediate full feeding, whereas 17 patients initially used the gastrostomy to supplement oral intake, 4 for medication administration and 1 for hydration. Initially the PEG regime met 73% ± 31% of the estimated total energy requirements, increasing to 87% ± 32% prior to death. There was stabilization of weight in patients undergoing gastrostomy [BMI at 3 mo (22.6 ± 2.2 kg/m(2)) and 6 mo (22.5 ± 2.0 kg/m(2)) after PEG placement compared to weight at the time of the procedure (22.5 ± 3.0 kg/m(2))]. However, weight loss recurred in the terminal stages of the illness. There was a strong trend for longer survival from diagnosis among MND in PEG recipients with limb onset presentation compared to similar patients who did not undergo the procedure (P = 0.063). Initial discussions regarding PEG insertion occurred earlier after diagnosis when seen by nutrition support team (NST) clinicians compared to other clinicians. (5.4 ± 7.0 mo vs 11.9 ± 13.4 mo, P = 0.028). There was a significant increase in PEG uptake (56% vs 24%, P = 0.011) if PEG discussions were initiated by the NST staff compared to other clinicians. There was no change in the ALSFRS-R score in patients who underwent PEG (pre 34.1 ± 8.6 vs post 34.8 ± 7.4), although in non-PEG recipients there was a non-significant fall in this score (33.7 ± 7.9 vs 31.6 ± 8.8). Four patients died within one month of the procedure, 4 developed bacterial site infection requiring antibiotics and 1 required endoscopic therapy for gastric bleeding. Less serious complications attributed to the procedure included persistent gastrostomy site discomfort, poor appetite, altered bowel function and bloating.
Conclusion: Initial discussion with NST clinicians increases PEG uptake in MND. Gastrostomy stabilizes patient weight but weight loss recurs with advancing disease.
Keywords: Motor neuron disease; Multidisciplinary management; Nutrition support team; Percutaneous endoscopic gastrostomy; Survival.
Figures
References
-
- Mazzini L, Corrà T, Zaccala M, Mora G, Del Piano M, Galante M. Percutaneous endoscopic gastrostomy and enteral nutrition in amyotrophic lateral sclerosis. J Neurol. 1995;242:695–698. - PubMed
-
- Forbes RB, Colville S, Swingler RJ. Frequency, timing and outcome of gastrostomy tubes for amyotrophic lateral sclerosis/motor neurone disease--a record linkage study from the Scottish Motor Neurone Disease Register. J Neurol. 2004;251:813–817. - PubMed
-
- Strong MJ, Rowe A, Rankin RN. Percutaneous gastrojejunostomy in amyotrophic lateral sclerosis. J Neurol Sci. 1999;169:128–132. - PubMed
-
- Chiò A, Finocchiaro E, Meineri P, Bottacchi E, Schiffer D. Safety and factors related to survival after percutaneous endoscopic gastrostomy in ALS. ALS Percutaneous Endoscopic Gastrostomy Study Group. Neurology. 1999;53:1123–1125. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
