

Risk clinicopathological factors for lymph node metastasis in poorly differentiated early gastric cancer and their impact on laparoscopic wedge resection
- PMID: 23197896
- PMCID: PMC3508645
- DOI: 10.3748/wjg.v18.i44.6489
Risk clinicopathological factors for lymph node metastasis in poorly differentiated early gastric cancer and their impact on laparoscopic wedge resection
Abstract
Aim: To investigate the predictive factors of lymph node metastasis (LNM) in poorly differentiated early gastric cancer (EGC), and enlarge the possibility of using laparoscopic wedge resection (LWR).
Methods: We retrospectively analyzed 85 patients with poorly differentiated EGC who underwent surgical resection between January 1992 and December 2010. The association between the clinicopathological factors and the presence of LNM was retrospectively analyzed by univariate and multivariate logistic regression analyses. Odds ratios (OR) with 95%CI were calculated. We further examined the relationship between the positive number of the three significant predictive factors and the LNM rate.
Results: In the univariate analysis, tumor size (P = 0.011), depth of invasion (P = 0.007) and lymphatic vessel involvement (P < 0.001) were significantly associated with a higher rate of LNM. In the multivariate model, tumor size (OR = 7.125, 95%CI: 1.251-38.218, P = 0.041), depth of invasion (OR = 16.624, 95%CI: 1.571-82.134, P = 0.036) and lymphatic vessel involvement (OR = 39.112, 95%CI: 1.745-123.671, P = 0.011) were found to be independently risk clinicopathological factors for LNM. Of the 85 patients diagnosed with poorly differentiated EGC, 12 (14.1%) had LNM. The LNM rates were 5.7%, 42.9% and 57.1%, respectively in cases with one, two and three of the risk factors respectively in poorly differentiated EGC. There was no LNM in 29 patients without the three risk clinicopathological factors.
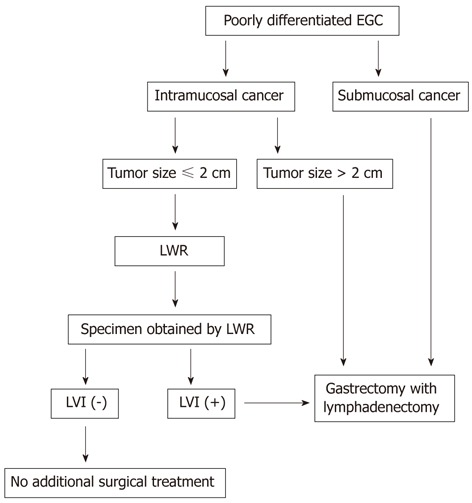
Conclusion: LWR alone may be sufficient treatment for intramucosal poorly differentiated EGC if the tumor is less than or equal to 2.0 cm in size, and when lymphatic vessel involvement is absent at postoperative histological examination.
Keywords: Clinicopathological characteristics; Early gastric cancer; Laparoscopic wedge resection; Lymph node metastasis; Poorly differentiated early gastric cancer.
Figures
References
-
- Kitaoka H, Yoshikawa K, Hirota T, Itabashi M. Surgical treatment of early gastric cancer. Jpn J Clin Oncol. 1984;14:283–293. - PubMed
-
- Koeda K, Nishizuka S, Wakabayashi G. Minimally invasive surgery for gastric cancer: the future standard of care. World J Surg. 2011;35:1469–1477. - PubMed
-
- Nozaki I, Kubo Y, Kurita A, Tanada M, Yokoyama N, Takiyama W, Takashima S. Long-term outcome after laparoscopic wedge resection for early gastric cancer. Surg Endosc. 2008;22:2665–2669. - PubMed
-
- Etoh T, Shiraishi N, Kitano S. Laparoscopic gastrectomy for cancer. Dig Dis. 2005;23:113–118. - PubMed
-
- Kitano S, Shiraishi N. Current status of laparoscopic gastrectomy for cancer in Japan. Surg Endosc. 2004;18:182–185. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
