

Automated telephone calls to enhance colorectal cancer screening: economic analysis
- PMID: 23198712
- PMCID: PMC3845657
Automated telephone calls to enhance colorectal cancer screening: economic analysis
Abstract
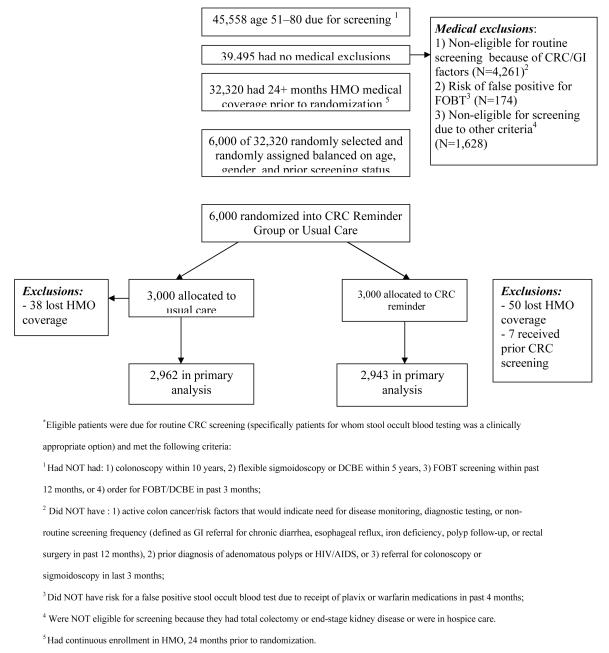
Objectives: To estimate the cost-effectiveness of an automated telephone intervention for colorectal cancer screening from a managed care perspective, using data from a pragmatic randomized controlled trial.
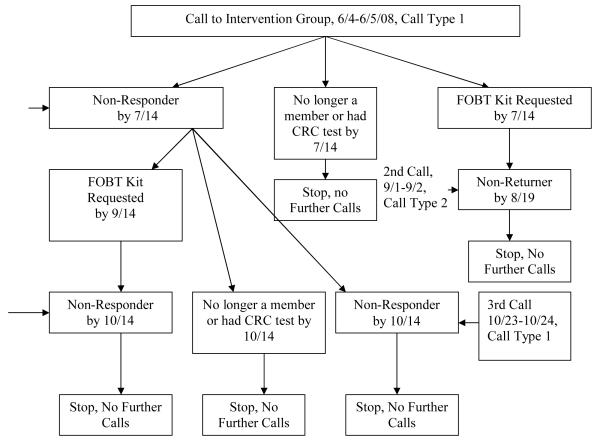
Methods: Intervention patients received calls for fecal occult blood testing (FOBT) screening. We searched patients' electronic medical records for any screening (defined as FOBT, flexible sigmoidoscopy, double-contrast barium enema, or colonoscopy) during follow-up. Intervention costs included project implementation and management, telephone calls, patient identification, and tracking. Screening costs included FOBT (kits, mailing, and processing) and any completed screening tests during follow-up. We estimated the incremental cost-effectiveness ratio (ICER) of the cost per additional screen.
Results: At 6 months, average costs for intervention and control patients were $37 (25% screened) and $34 (19% screened), respectively. The ICER at 6 months was $42 per additional screen, less than half what other studies have reported. Cost-effectiveness probability was 0.49, 0.84, and 0.99 for willingness-to-pay thresholds of $40, $100, and $200, respectively. Similar results were seen at 9 months. A greater increase in FOBT testing was seen for patients aged >70 years (45/100 intervention, 33/100 control) compared with younger patients (25/100 intervention, 21/100 control). The intervention was dominant for patients aged >70 years and was $73 per additional screen for younger patients. It increased screening rates by about 6% and costs by $3 per patient.
Conclusions: At willingness to pay of $100 or more per additional screening test, an automated telephone reminder intervention can be an optimal use of resources.
Figures
References
-
- Altekruse SF, Kosary CL, Krapcho M, Neyman N, Aminou R, Waldron W, Ruhl J, Howlader N, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Cronin K, Chen HS, Feuer EJ, Stinchcomb DG, Edwards BK, editors. World Wide Web. National Cancer Institute; Bethesda, MD: 2010. SEER Cancer Statistics Review, 1975-2007. http://seer.cancer.gov/csr/1975_2007/ based on November 2009 SEER data submission, posted to the SEER web site.
-
- Sun Hee Rim, Joseph Djenaba A, Steele Brooke, Thompson Trevor D, Seeff Laura C. Colorectal Cancer Screening --- United States, 2002, 2004, 2006, and 2008. MMWR Morb Mortal Wkly Rep. 2011;60:42–46. - PubMed
-
- Lairson DR, DiCarlo M, Myers RE, et al. Cost-effectiveness of targeted and tailored interventions on colorectal cancer screening use. Cancer. 2008;112:779–788. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
