

Birth asphyxia as the major complication in newborns: moving towards improved individual outcomes by prediction, targeted prevention and tailored medical care
- PMID: 23199149
- PMCID: PMC3405378
- DOI: 10.1007/s13167-011-0087-9
Birth asphyxia as the major complication in newborns: moving towards improved individual outcomes by prediction, targeted prevention and tailored medical care
Abstract
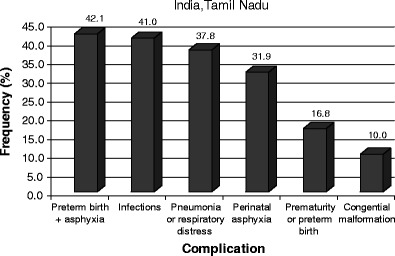
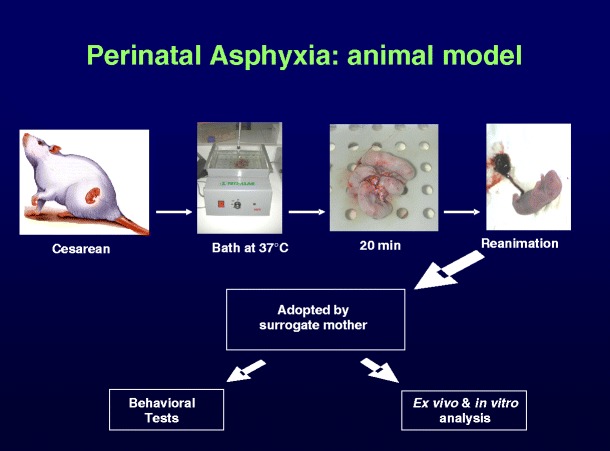
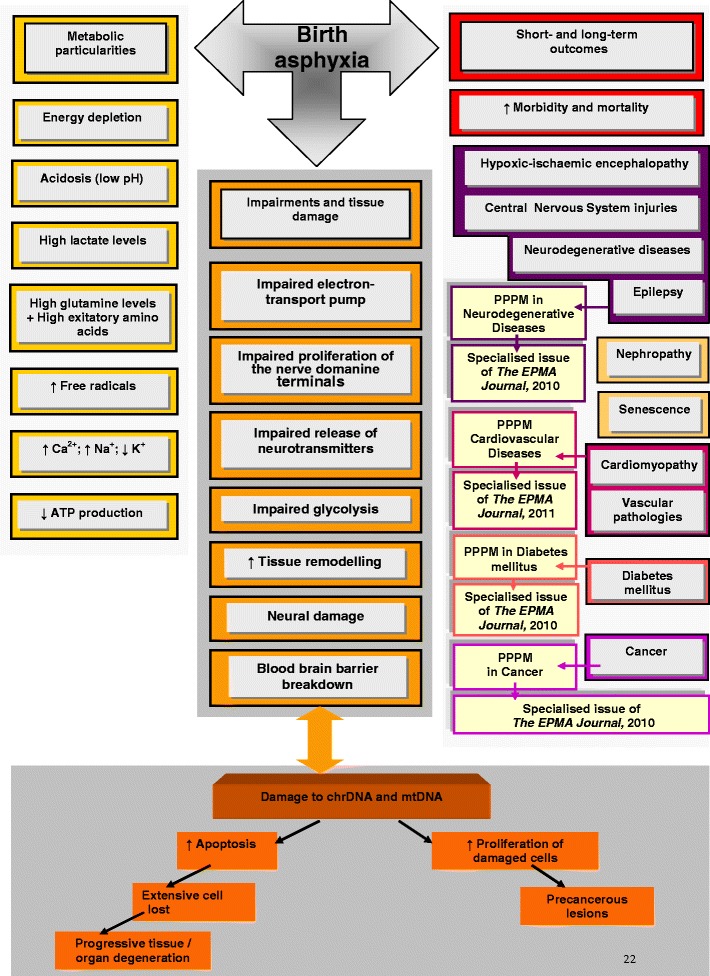
Perinatal Asphyxia-oxygen deficit at delivery-can lead to severe hypoxic ischaemic organ damage in newborns followed by a fatal outcome or severe life-long pathologies. The severe insults often cause neurodegenerative diseases, mental retardation and epilepsies. The mild insults lead to so-called "minimal brain-damage disorders" such as attention deficits and hyperactivity, but can also be associated with the development of schizophrenia and life-long functional psychotic syndromes. Asphyxia followed by re-oxygenation can potentially lead to development of several neurodegenerative pathologies, diabetes type 2 and cancer. The task of individual prediction, targeted prevention and personalised treatments before a manifestation of the life-long chronic pathologies usually developed by newborns with asphyxic deficits, should be given the extraordinary priority in neonatology and paediatrics. Socio-economical impacts of educational measures and advanced strategies in development of robust diagnostic approaches targeted at effected molecular pathways, biomarker-candidates and potential drug-targets for tailored treatments are reviewed in the paper.
Figures

References
-
- Peeva V, Golubnitschaja O. Birth asphyxia as the most frequent perinatal complication. In: Golubnitschaja O, editor. Predictive diagnostics and personalized treatment: dream or reality? New York: Nova Science Publishers; 2009. pp. 499–507.
-
- Tomashek KM, Crouse CJ, Iyasu S, Johnson CH, Flowers LM. A comparison of morbidity rates attributable to conditions originating in the perinatal period among newborns discharged from United States hospitals, 1989–90 and 1999–2000. Paediatr Perinat Epidemiol. 2006;20:24–34. doi: 10.1111/j.1365-3016.2006.00690.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
