

Modeling the impact of public access defibrillator range on public location cardiac arrest coverage
- PMID: 23201501
- PMCID: PMC3615148
- DOI: 10.1016/j.resuscitation.2012.11.019
Modeling the impact of public access defibrillator range on public location cardiac arrest coverage
Abstract
Background: Public access defibrillation with automated external defibrillators (AEDs) can improve survival from out-of-hospital cardiac arrests (OHCA) occurring in public. Increasing the effective range of AEDs may improve coverage for public location OHCAs.
Objective: To quantify the relationship between AED effective range and public location cardiac arrest coverage.
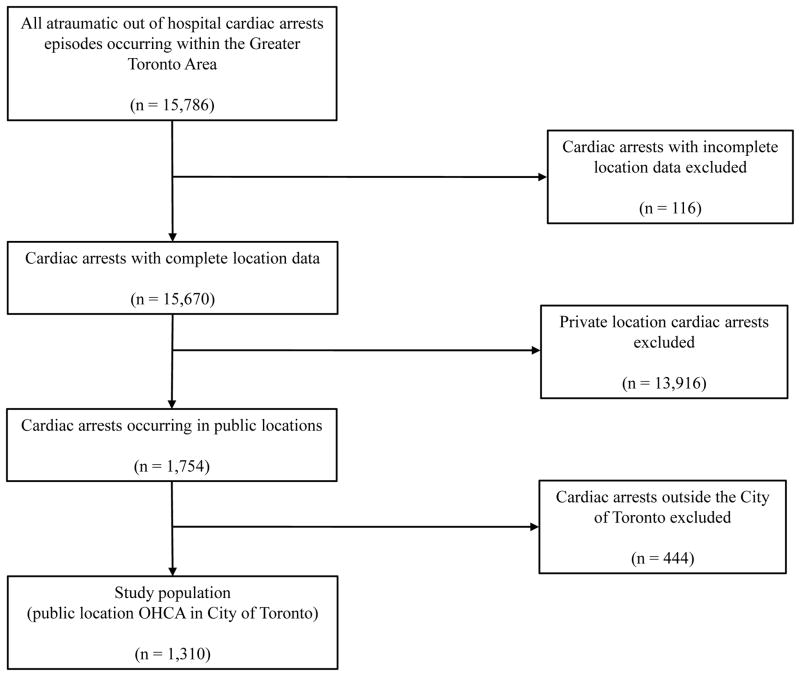
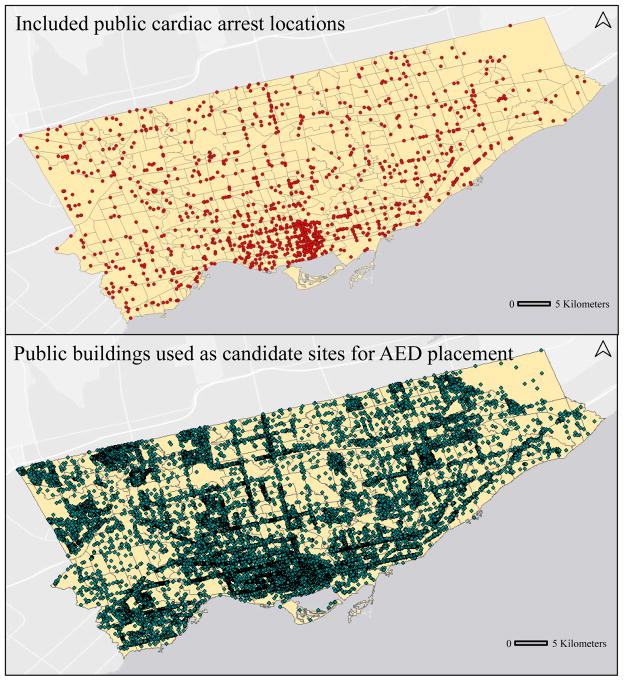
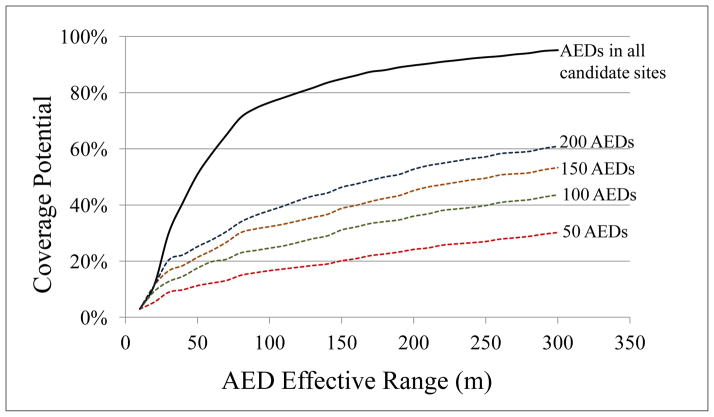
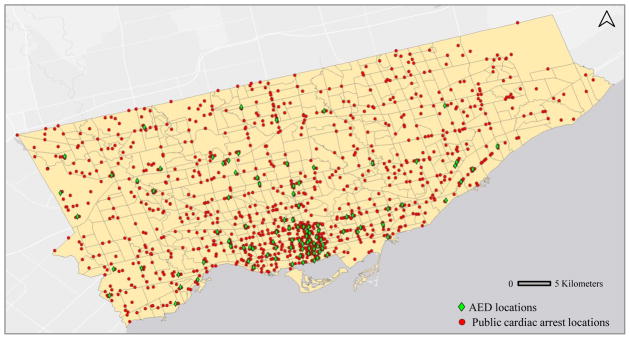
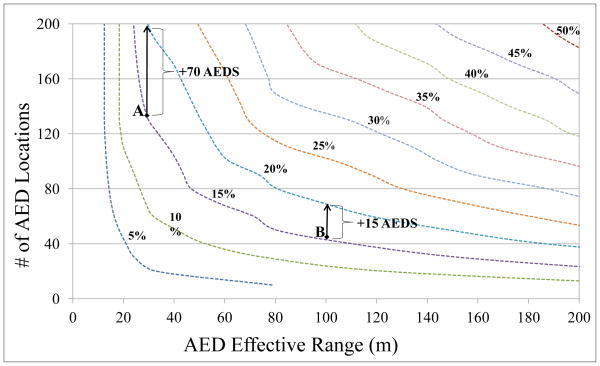
Methods: This was a retrospective cohort study using the Resuscitation Outcomes Consortium Epistry database. We included all public-location, atraumatic, EMS-attended OHCAs in Toronto, Canada between December 16, 2005 and July 15, 2010. We ran a mathematical model for AED placement that maximizes coverage of historical public OHCAs given pre-specified values of AED effective range and the number of locations to place AEDs. Locations of all non-residential buildings were obtained from the City of Toronto and used as candidate sites for AED placement. Coverage was evaluated for range values from 10 to 300 m and number of AED locations from 10 to 200, both in increments of 10, for a total of 600 unique scenarios. Coverage from placing AEDs in all public buildings was also measured.
Results: There were 1310 public location OHCAs during the study period, with 25,851 non-residential buildings identified as candidate sites for AED placement. Cardiac arrest coverage increased with AED effective range, with improvements in coverage diminishing at higher ranges. For example, for a deployment of 200 AED locations, increasing effective range from 100 m to 200 m covered an additional 15% of cardiac arrests, whereas increasing range further from 200 m to 300 m covered an additional 10%. Placing an AED in each of the 25,851 public buildings resulted in coverage of 50% and 95% under assumed effective ranges of 50 m and 300 m, respectively.
Conclusion: Increasing AED effective range can improve cardiac arrest coverage. Mathematical models can help evaluate the potential impact of initiatives which increase AED range.
Copyright © 2012 Elsevier Ireland Ltd. All rights reserved.
Figures
Similar articles
-
Overcoming Spatial and Temporal Barriers to Public Access Defibrillators Via Optimization.J Am Coll Cardiol. 2016 Aug 23;68(8):836-45. doi: 10.1016/j.jacc.2016.03.609. J Am Coll Cardiol. 2016. PMID: 27539176 Free PMC article. Clinical Trial.
-
Identifying locations for public access defibrillators using mathematical optimization.Circulation. 2013 Apr 30;127(17):1801-9. doi: 10.1161/CIRCULATIONAHA.113.001953. Epub 2013 Apr 3. Circulation. 2013. PMID: 23553657
-
Effect of Optimized Versus Guidelines-Based Automated External Defibrillator Placement on Out-of-Hospital Cardiac Arrest Coverage: An In Silico Trial.J Am Heart Assoc. 2020 Sep;9(17):e016701. doi: 10.1161/JAHA.120.016701. Epub 2020 Aug 20. J Am Heart Assoc. 2020. PMID: 32814479 Free PMC article. Clinical Trial.
-
The challenges and possibilities of public access defibrillation.J Intern Med. 2018 Mar;283(3):238-256. doi: 10.1111/joim.12730. Epub 2018 Feb 12. J Intern Med. 2018. PMID: 29331055 Review.
-
Public access defibrillation: challenges and new solutions.Curr Opin Crit Care. 2023 Jun 1;29(3):168-174. doi: 10.1097/MCC.0000000000001051. Epub 2023 Apr 24. Curr Opin Crit Care. 2023. PMID: 37093002 Free PMC article. Review.
Cited by
-
Ranking Businesses and Municipal Locations by Spatiotemporal Cardiac Arrest Risk to Guide Public Defibrillator Placement.Circulation. 2017 Mar 21;135(12):1104-1119. doi: 10.1161/CIRCULATIONAHA.116.025349. Circulation. 2017. PMID: 28320803 Free PMC article.
-
Overcoming Spatial and Temporal Barriers to Public Access Defibrillators Via Optimization.J Am Coll Cardiol. 2016 Aug 23;68(8):836-45. doi: 10.1016/j.jacc.2016.03.609. J Am Coll Cardiol. 2016. PMID: 27539176 Free PMC article. Clinical Trial.
-
Identifying the relative importance of predictors of survival in out of hospital cardiac arrest: a machine learning study.Scand J Trauma Resusc Emerg Med. 2020 Jun 25;28(1):60. doi: 10.1186/s13049-020-00742-9. Scand J Trauma Resusc Emerg Med. 2020. PMID: 32586339 Free PMC article.
-
Comparative Analysis of Out-of-Hospital Cardiac Arrest Outcomes in Health Clinics, Nursing Homes, and Public Places: Implications for Optimizing Automated External Defibrillator Strategies.Int J Gen Med. 2024 May 18;17:2241-2249. doi: 10.2147/IJGM.S464936. eCollection 2024. Int J Gen Med. 2024. PMID: 38779653 Free PMC article.
-
The Role of Automated External Defibrillator Use in the Out-of-Hospital Cardiac Arrest Survival Rate and Outcome: A Systematic Review.Cureus. 2023 Oct 26;15(10):e47721. doi: 10.7759/cureus.47721. eCollection 2023 Oct. Cureus. 2023. PMID: 38021997 Free PMC article. Review.
References
-
- Weisfeldt ML, Sitlani CM, Ornato JP, Rea T, Aufderheide TP, Davis D, Dreyer J, Hess EP, Jui J, Maloney J, Sopko G, Powell J, Nichol G, Morrison LJ for the ROC Investigators. Survival after application of automatic external defibrillators before arrival of the emergency medical system: Evaluation in the Resuscitation Outcomes Consortium population of 21 million. J Am Coll Cardiol. 2010;55:1713–1720. - PMC - PubMed
-
- Nichol G, Stiell IG, Laupacis A, et al. A Cumulative metaanalysis of the effectiveness of defibrillator-capable emergency medical services for victims of out-of-hospital cardiac arrest. Ann Emerg Med. 1999;34:517–525. - PubMed
-
- Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. N Engl J Med. 2000;343:1206–1209. - PubMed
-
- Page RL, Joglar JA, Kowal RC, Zagrodzky JD, Nelson LL, Ramaswamy K, Barbera SJ, Hamdan MH, McKenas DK. Use of automated external defibrillators by a U.S. airline. New Engl J Med. 2000;343:1210–1216. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL077866/HL/NHLBI NIH HHS/United States
- U01 HL077885/HL/NHLBI NIH HHS/United States
- CAPMC/ CIHR/Canada
- HL077867/HL/NHLBI NIH HHS/United States
- 5U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077881/HL/NHLBI NIH HHS/United States
- U01 HL077872/HL/NHLBI NIH HHS/United States
- HL077871/HL/NHLBI NIH HHS/United States
- HL077881/HL/NHLBI NIH HHS/United States
- HL077908/HL/NHLBI NIH HHS/United States
- U01 HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077908/HL/NHLBI NIH HHS/United States
- HL077866/HL/NHLBI NIH HHS/United States
- HL077872/HL/NHLBI NIH HHS/United States
- HL077863/HL/NHLBI NIH HHS/United States
- U01 HL077867/HL/NHLBI NIH HHS/United States
- HL077885/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
