

Is bilateral lymphadenectomy for midline squamous carcinoma of the vulva always necessary? An analysis from Gynecologic Oncology Group (GOG) 173
- PMID: 23201592
- PMCID: PMC3638213
- DOI: 10.1016/j.ygyno.2012.11.034
Is bilateral lymphadenectomy for midline squamous carcinoma of the vulva always necessary? An analysis from Gynecologic Oncology Group (GOG) 173
Abstract
Objective: To determine which patients with near midline lesions may safely undergo unilateral groin dissection based on clinical exam and lymphoscintigraphy (LSG) results.
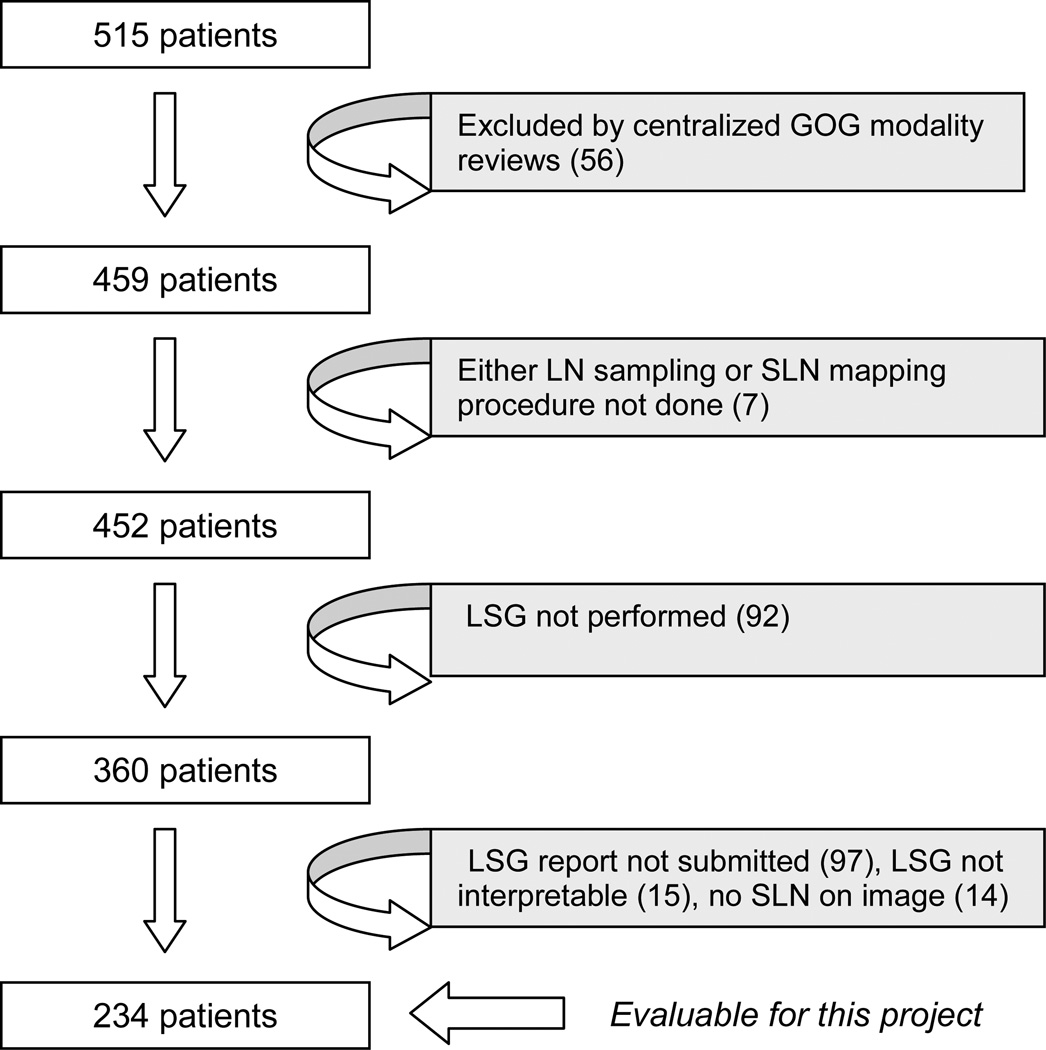
Methods: Patients participating in GOG-173 underwent sentinel lymph node (SLN) localization with blue dye, and radiocolloid with optional LSG before definitive inguinal-femoral lymphadenectomy (LND). This analysis interrogates the reliability of LSG alone relative to primary tumor location in those patients who had an interpretable LSG and at least one SLN identified. Primary tumor location was categorized as lateral (>2cm from midline), midline, or lateral ambiguous (LA) if located within 2cm, but not involving the midline.
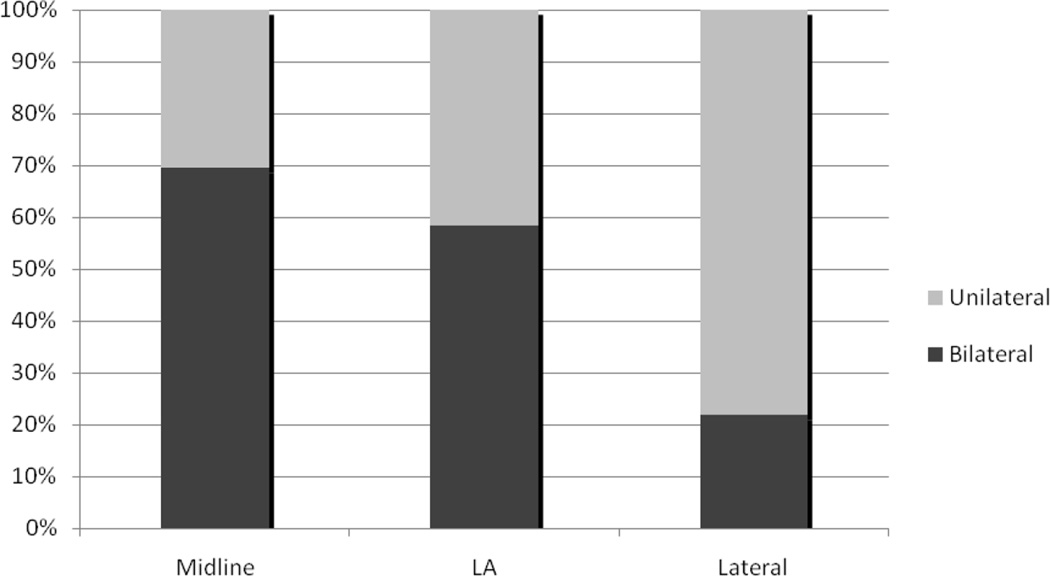
Results: Two-hundred-thirty-four patients met eligibility criteria. Sixty-four had lateral lesions, and underwent unilateral LND. All patients with LA (N=65) and midline (N=105) tumors underwent bilateral LND. Bilateral drainage by LSG was identified in 14/64 (22%) patients with lateral tumors, 38/65 (58%) with LA tumors and in 73/105 (70%) with midline tumors. At mapping, no SLNs were found in contralateral groins among those patients with LA and midline tumors who had unilateral-only LSGs. However, in these patients groin metastases were found in 4/32 patients with midline tumors undergoing contralateral dissection; none were found in 27 patients with LA tumors.
Conclusion: The likelihood of detectable bilateral drainage using preoperative LSG decreases as a function of distance from midline. Patients with LA primaries and unilateral drainage on LSG may safely undergo unilateral SLN.
Copyright © 2012 Elsevier Inc. All rights reserved.
Conflict of interest statement
Dr. Linda Van Le is on the Speaker’s Bureau for Eisai and the Advisory Board for Biologics, Inc. All other co-authors have no conflicts of interest to declare.
Figures
References
-
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. - PubMed
-
- Helm CW, Hatch K, Austin JM, Partridge EE, Soong SJ, Elder JE, et al. A matched comparison of single and triple incision techniques for the surgical treatment of carcinoma of the vulva. Gynecol Oncol. 1992;46:150–156. - PubMed
-
- Burke TW, Stringer CA, Gershenson DM, Edwards CL, Morris M, Wharton JT. Radical wide excision and selective inguinal node dissection for squamous cell carcinoma of the vulva. Gynecol Oncol. 1990;38:328–332. - PubMed
-
- Berman ML, Soper JT, Creasman WT, Olt GT, DiSaia PJ. Conservative surgical management of superficially invasive stage I vulvar carcinoma. Gynecol Oncol. 1989;35:352–357. - PubMed
-
- Lanza A, Valli M, Caldarola B, et al. Radical vulvectomy and inguinal lymphadenectomy versus inguino-pelvic lymphadenectomy combined with radical vulvectomy and the role of radiotherapy. Eur J Gynaec Oncol. 1988;9:67–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
