

An association between L-arginine/asymmetric dimethyl arginine balance, obesity, and the age of asthma onset phenotype
- PMID: 23204252
- PMCID: PMC3570651
- DOI: 10.1164/rccm.201207-1270OC
An association between L-arginine/asymmetric dimethyl arginine balance, obesity, and the age of asthma onset phenotype
Abstract
Rationale: Increasing body mass index (BMI) has been associated with less fractional exhaled nitric oxide (Fe(NO)). This may be explained by an increase in the concentration of asymmetric dimethyl arginine (ADMA) relative to L-arginine, which can lead to greater nitric oxide synthase uncoupling.
Objectives: To compare this mechanism across age of asthma onset groups and determine its association with asthma morbidity and lung function.
Methods: Cross-sectional study of participants from the Severe Asthma Research Program, across early- (<12 yr) and late- (>12 yr) onset asthma phenotypes.
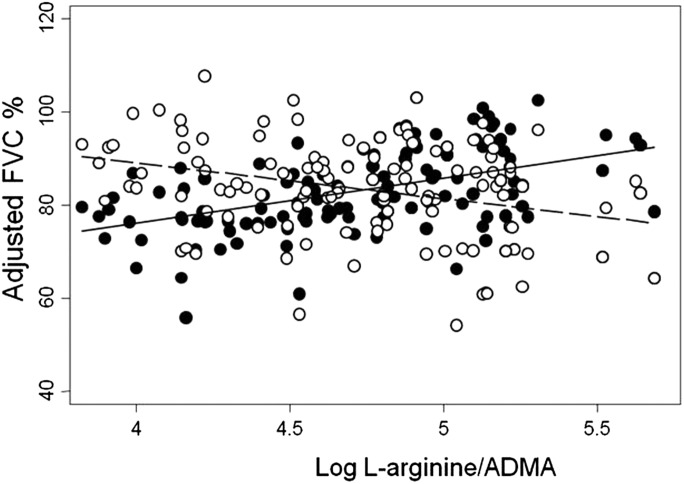
Measurements and main results: Subjects with late-onset asthma had a higher median plasma ADMA level (0.48 μM, [interquartile range (IQR), 0.35-0.7] compared with early onset, 0.37 μM [IQR, 0.29-0.59], P = 0.01) and lower median plasma l-arginine (late onset, 52.3 [IQR, 43-61] compared with early onset, 51 μM [IQR 39-66]; P = 0.02). The log of plasma L-arginine/ADMA was inversely correlated with BMI in the late- (r = -0.4, P = 0.0006) in contrast to the early-onset phenotype (r = -0.2, P = 0.07). Although Fe(NO) was inversely associated with BMI in the late-onset phenotype (P = 0.02), the relationship was lost after adjusting for L-arginine/ADMA. Also in this phenotype, a reduced L-arginine/ADMA was associated with less IgE, increased respiratory symptoms, lower lung volumes, and worse asthma quality of life.
Conclusions: In late-onset asthma phenotype, plasma ratios of L-arginine to ADMA may explain the inverse relationship of BMI to Fe(NO). In addition, these lower L-arginine/ADMA ratios are associated with reduced lung function and increased respiratory symptom frequency, suggesting a role in the pathobiology of the late-onset phenotype.
Figures






Comment in
-
Clinical-biological phenotyping beyond inflammation in asthma delivers.Am J Respir Crit Care Med. 2013 Jan 15;187(2):117-8. doi: 10.1164/rccm.201211-1978ED. Am J Respir Crit Care Med. 2013. PMID: 23322790 No abstract available.
References
-
- Berg CM, Thelle DS, Rosengren A, Lissner L, Torén K, Olin AC. Decreased fraction of exhaled nitric oxide in obese subjects with asthma symptoms: data from the population study INTERGENE/ADONIX. Chest 2011;139:1109–1116 - PubMed
-
- Barros R, Moreira A, Fonseca J, Moreira P, Fernandes L, de Oliveira JF, Delgado L, Castel-Branco MG. Obesity and airway inflammation in asthma. J Allergy Clin Immunol 2006;117:1501–1502 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
