

Chronic bronchitis and chronic obstructive pulmonary disease
- PMID: 23204254
- PMCID: PMC4951627
- DOI: 10.1164/rccm.201210-1843CI
Chronic bronchitis and chronic obstructive pulmonary disease
Abstract
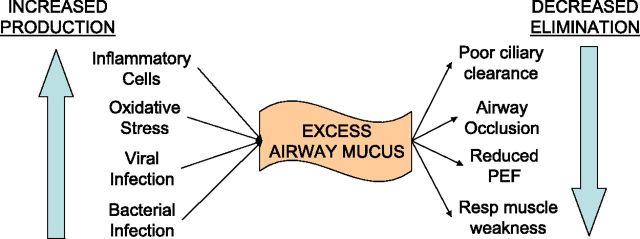
Chronic bronchitis (CB) is a common but variable phenomenon in chronic obstructive pulmonary disease (COPD). It has numerous clinical consequences, including an accelerated decline in lung function, greater risk of the development of airflow obstruction in smokers, a predisposition to lower respiratory tract infection, higher exacerbation frequency, and worse overall mortality. CB is caused by overproduction and hypersecretion of mucus by goblet cells, which leads to worsening airflow obstruction by luminal obstruction of small airways, epithelial remodeling, and alteration of airway surface tension predisposing to collapse. Despite its clinical sequelae, little is known about the pathophysiology of CB and goblet cell hyperplasia in COPD, and treatment options are limited. In addition, it is becoming increasingly apparent that in the classic COPD spectrum, with emphysema on one end and CB on the other, most patients lie somewhere in the middle. It is known now that many patients with severe emphysema can develop CB, and small airway pathology has been linked to worse clinical outcomes, such as increased mortality and lesser improvement in lung function after lung volume reduction surgery. However, in recent years, a greater understanding of the importance of CB as a phenotype to identify patients with a beneficial response to therapy has been described. Herein we review the epidemiology of CB, the evidence behind its clinical consequences, the current understanding of the pathophysiology of goblet cell hyperplasia in COPD, and current therapies for CB.
Figures
References
-
- Mathers CD, Bernard C, Iburg KM, Inoue M, Fat DM, Shibuya K, Stein C, Tomijima N, Xu H. Global Burden of Disease in 2002: data sources, methods and results. Geneva, Switzerland: World Health Organization; 2003. Global Programme on Evidence for Health Policy Discussion Paper No. 54.
-
- National Heart Lung and Blood Institute, National Institutes of Health. Global Initiative for Chronic Obstructive Lung Disease (GOLD) guidelines, global strategy for the diagnosis, management and prevention of chronic obstructive lung disease: NHLBI/WHO workshop report. Bethesda, MD: NIH; 2001. NIH publication 2701.
-
- Vestbo J, Prescott E, Lange P. Association of chronic mucus hypersecretion with FEV1 decline and chronic obstructive pulmonary disease morbidity. Copenhagen City Heart Study Group. Am J Respir Crit Care Med 1996;153:1530–1535. - PubMed
-
- Burgel PR, Nesme-Meyer P, Chanez P, Caillaud D, Carre P, Perez T, Roche N, Initiatives Bronchopneumopathie Chronique Obstructive Scientific Committee. Cough and sputum production are associated with frequent exacerbations and hospitalizations in COPD subjects. Chest 2009;135:975–982. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
