

Ureteral interventions
- PMID: 23204637
- PMCID: PMC3312173
- DOI: 10.1055/s-0031-1296081
Ureteral interventions
Abstract
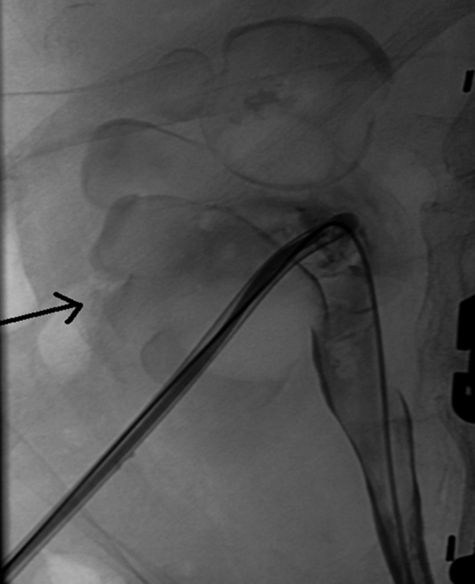
The pelvic course of the ureter with its close proximity to the iliac artery, pelvic viscera, and other structures predispose to fistula formation. Surgical management of lower urinary tract fistulas is difficult and often ineffective. Nonvascular lower urinary tract fistulas can be managed by urinary diversion with percutaneous nephrostomy to allow for fistula healing. If this fails, ureteral embolization can be very effective; however, this should be preceded by careful evaluation and discussion with the patient as this intervention results in irreversible ureteral occlusion necessitating a diverting nephrostomy catheter indefinitely. A ureteroarterial fistula is a distinct entity compared with nonvascular fistulas with a different approach to management; it can be managed by exclusion of the fistula by endovascular placement of a stent graft across the arterial component of the fistula.
Keywords: Fistula; embolization; kidney; nephrostomy; ureter.
Figures






References
-
- Avritscher R, Madoff D C, Ramirez P T, et al. Fistulas of the lower urinary tract: Percutaneous approaches for the management of a difficult clinical entity. Radiographics. 2004;24(suppl 1):S217–S236. - PubMed
-
- Bing K T, Hicks M E, Figenshau R S, et al. Percutaneous ureteral occlusion with use of Gianturco coils and gelatin sponge. Part I. Swine model. J Vasc Interv Radiol. 1992a;3(2):313–317. - PubMed
-
- Bing K T, Hicks M E, Picus D, Darcy M D. Percutaneous ureteral occlusion with use of Gianturco coils and gelatin sponge. Part II. Clinical experience. J Vasc Interv Radiol. 1992;3(2):319–321. - PubMed
-
- Shindel A W, Zhu H, Hovsepian D M, Brandes S B. Ureteric embolization with stainless-steel coils for managing refractory lower urinary tract fistula: a 12-year experience. BJU Int. 2007;99(2):364–368. - PubMed
-
- Adamo R, Saad WEA, Brown D B. Percutaneous ureteral interventions. Tech Vasc Interv Radiol. 2009;12(3):205–215. - PubMed
