

The role of interventional radiology in urologic tract trauma
- PMID: 23204640
- PMCID: PMC3312175
- DOI: 10.1055/s-0031-1296084
The role of interventional radiology in urologic tract trauma
Abstract
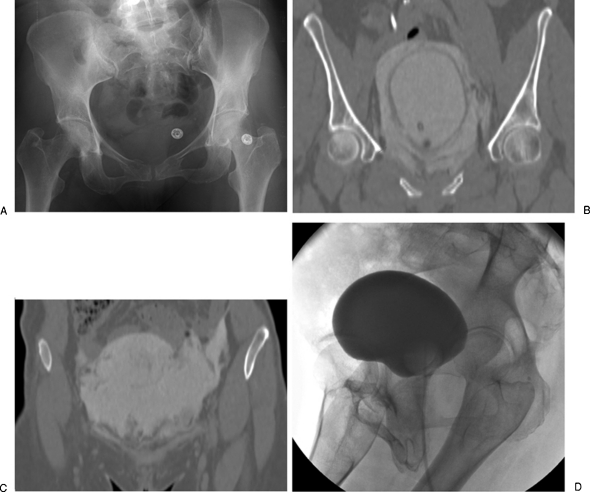
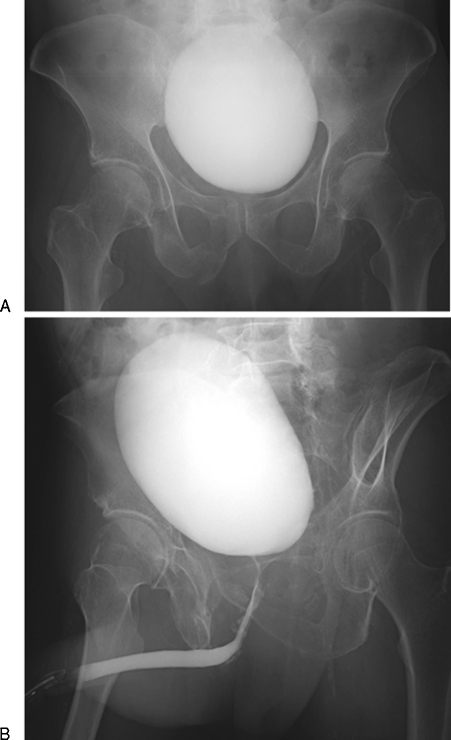
The kidney is the third most common abdominal organ to be injured in trauma, following the spleen and liver, respectively. Several classification systems convey the severity of injury to kidneys, ureter, bladder, and urethra. The most commonly used classification scheme is the American Association for the Surgery of Trauma (AAST) classification of blunt renal injuries, which grades renal injury according the size of laceration and its proximity to the renal hilum. Ureteral injury is graded according to its extent relative to the circumference of the ureter and the extent of associated devascularization. Bladder injury is graded according to its location relative to the peritoneum. Urethral injury is graded according to the extent of damage to surrounding anatomic structures. Although these classification schema may not be always used in common parlance, they do help delineate most important features of urologic tract injury that impact patient management and interventions.
Keywords: Kidney; embolization; genitourinary; interventional radiology; trauma.
Figures
Comment in
-
Re: The role of interventional radiology in urologic tract trauma.J Urol. 2013 Oct;190(4):1298. doi: 10.1016/j.juro.2013.06.044. Epub 2013 Jun 21. J Urol. 2013. PMID: 24029329 No abstract available.
References
-
- Titton R L, Gervais D A, Boland G W, Mueller P R. Renal trauma: radiologic evaluation and percutaneous treatment of nonvascular injuries. AJR Am J Roentgenol. 2002;178(6):1507–1511. - PubMed
-
- Bixby S D, Callahan M J, Taylor G A. Imaging blunt pediatric blunt abdominal trauma. Semin Roentgenol. 2008;43(1):72–82. - PubMed
-
- McAleer I M, Kaplan G W, LoSasso B E. Congenital urinary tract anomalies in pediatric renal trauma patients. J Urol. 2002;168(4 Pt 2):1808–1810. discussion 1810. - PubMed
-
- Lorelli D R, Kralovich K A, Seguin C. The impact of pre-existing end-stage renal disease on survival in acutely injured trauma patients. Am Surg. 2001;67(7):693–696. - PubMed
-
- Patel M S, Malinoski D J, Nguyen X M, Hoyt D B. The impact of select chronic diseases on outcomes after trauma: a study from the National Trauma Data Bank. J Am Coll Surg. 2011;212(1):96–104. - PubMed
