

Sedation in the intensive care setting
- PMID: 23204873
- PMCID: PMC3508653
- DOI: 10.2147/CPAA.S26582
Sedation in the intensive care setting
Abstract
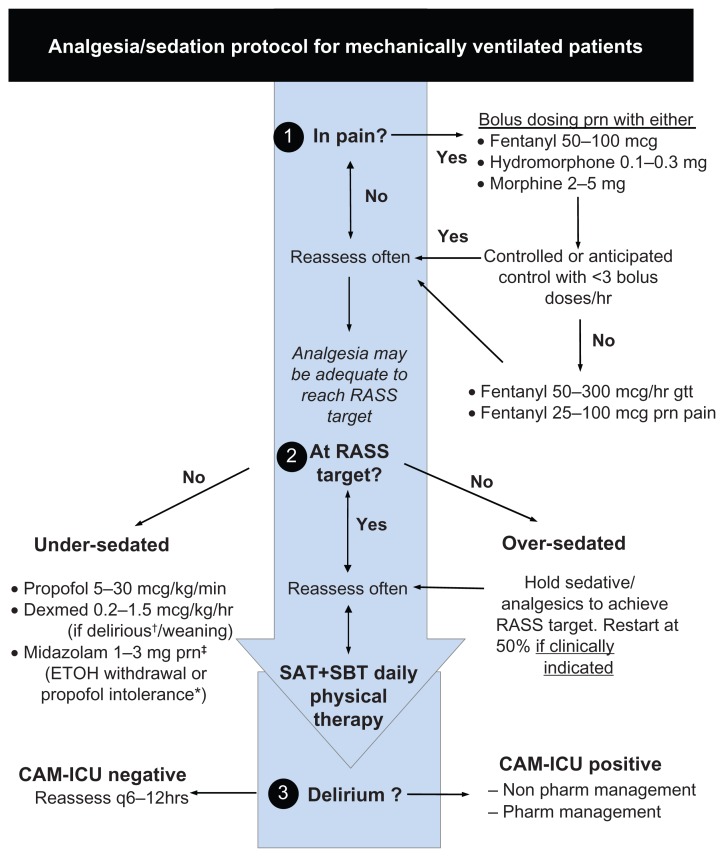
Critically ill patients are routinely provided analgesia and sedation to prevent pain and anxiety, permit invasive procedures, reduce stress and oxygen consumption, and improve synchrony with mechanical ventilation. Regional preferences, patient history, institutional bias, and individual patient and practitioner variability, however, create a wide discrepancy in the approach to sedation of critically ill patients. Untreated pain and agitation increase the sympathetic stress response, potentially leading to negative acute and long-term consequences. Oversedation, however, occurs commonly and is associated with worse clinical outcomes, including longer time on mechanical ventilation, prolonged stay in the intensive care unit, and increased brain dysfunction (delirium and coma). Modifying sedation delivery by incorporating analgesia and sedation protocols, targeted arousal goals, daily interruption of sedation, linked spontaneous awakening and breathing trials, and early mobilization of patients have all been associated with improvements in patient outcomes and should be incorporated into the clinical management of critically ill patients. To improve outcomes, including time on mechanical ventilation and development of acute brain dysfunction, conventional sedation paradigms should be altered by providing necessary analgesia, incorporating propofol or dexmedetomidine to reach arousal targets, and reducing benzodiazepine exposure.
Keywords: Behavioral Pain Scale; Confusion Assessment Method for the ICU; Richmond Agitation-Sedation Scale; Sedation-Agitation Scale; dexmedetomidine; fentanyl; propofol.
Figures
References
-
- Jacobi J, Fraser GL, Coursin DB, et al. Clinical practice guidelines for the sustained use of sedatives and analgesics in the critically ill adult. Crit Care Med. 2002;30(1):119–141. - PubMed
-
- Kapfhammer HP, Rothenhausler HB, Krauseneck T, Stoll C, Schelling G. Posttraumatic stress disorder and health-related quality of life in long-term survivors of acute respiratory distress syndrome. Am J Psychiatry. 2004;161(1):45–52. - PubMed
-
- Kollef MH, Levy NT, Ahrens TS, Schaiff R, Prentice D, Sherman G. The use of continuous i.v. sedation is associated with prolongation of mechanical ventilation. Chest. 1998;114(2):541–548. - PubMed
-
- Pandharipande P, Shintani A, Peterson J, et al. Lorazepam is an independent risk factor for transitioning to delirium in intensive care unit patients. Anesthesiology. 2006;104(1):21–26. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
