

The relative impact of circumferential and longitudinal shortening on left ventricular ejection fraction and stroke volume
- PMID: 23204893
- PMCID: PMC3383360
The relative impact of circumferential and longitudinal shortening on left ventricular ejection fraction and stroke volume
Abstract
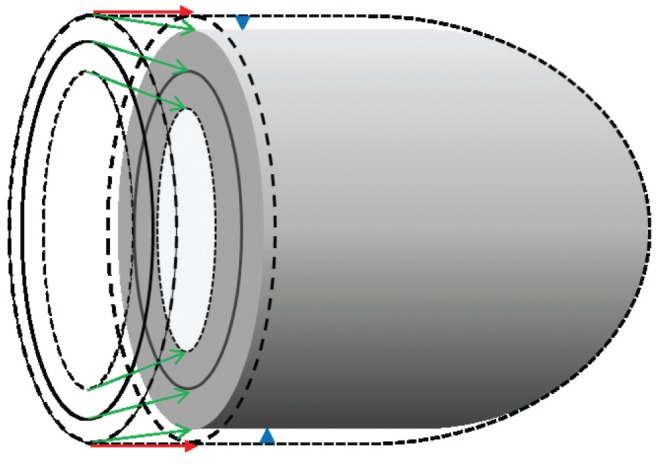
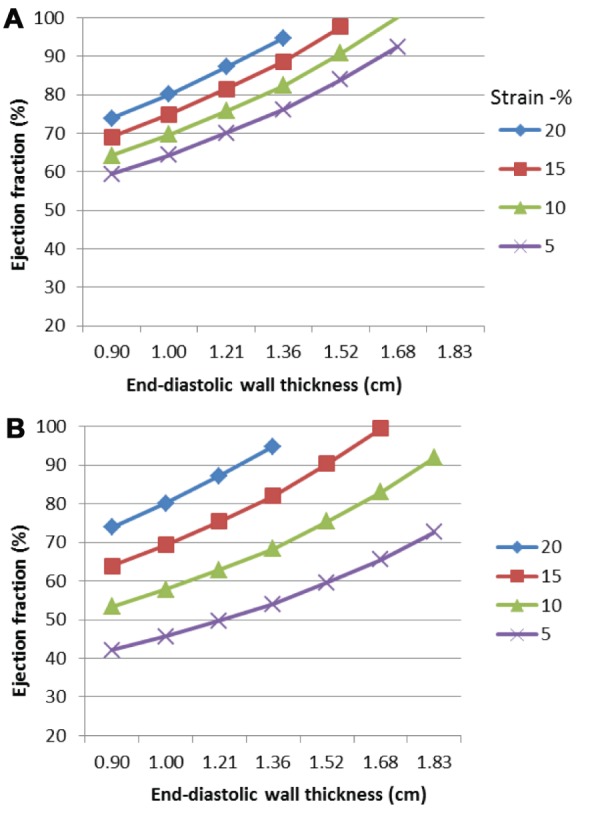
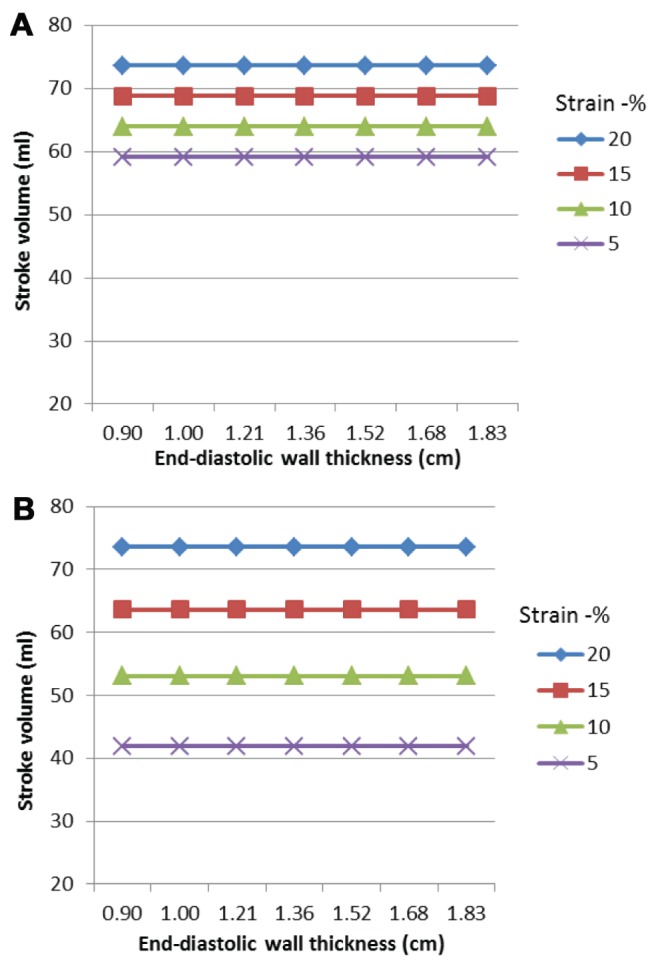
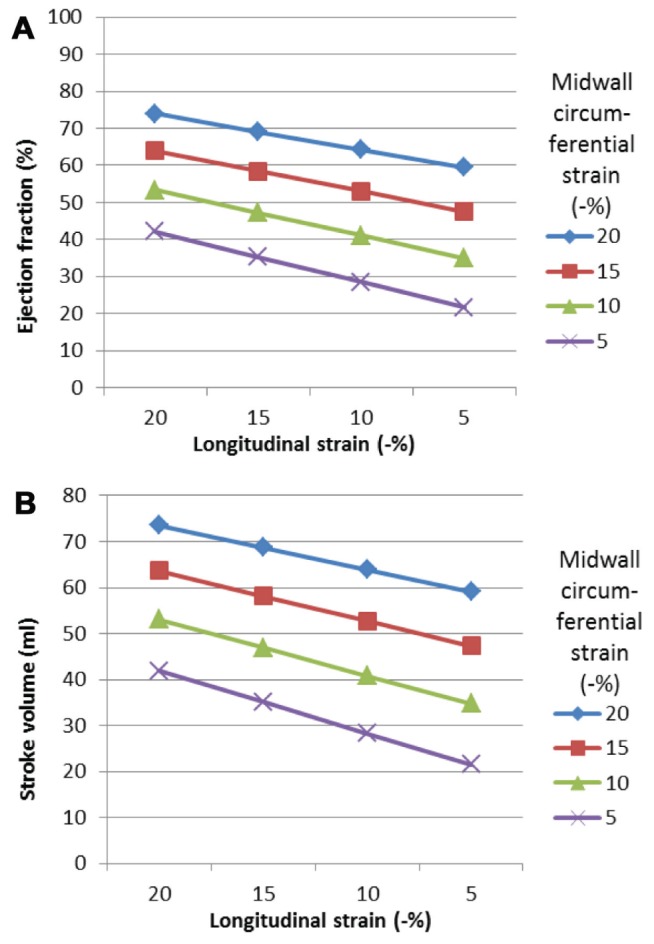
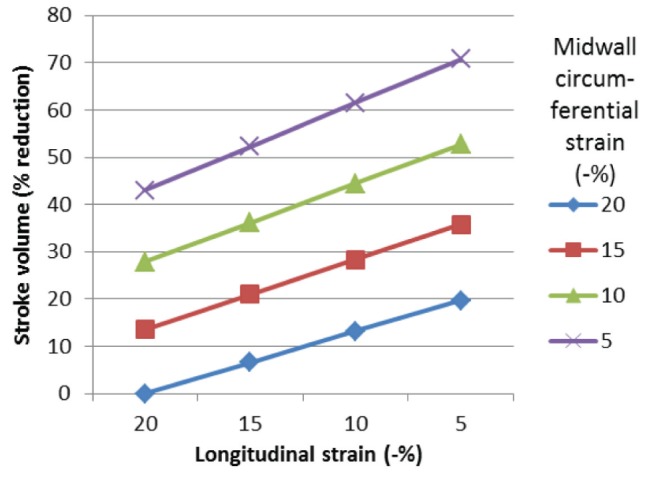
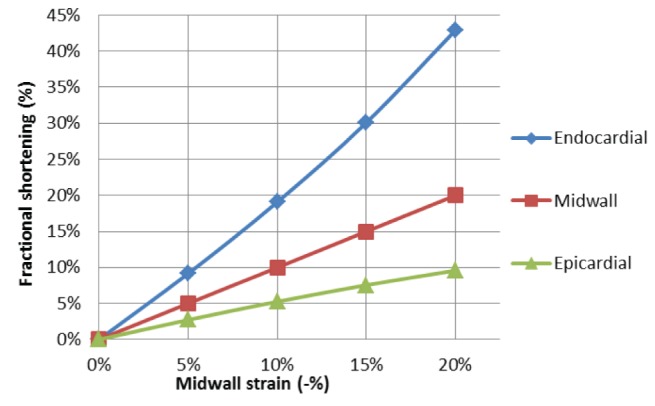
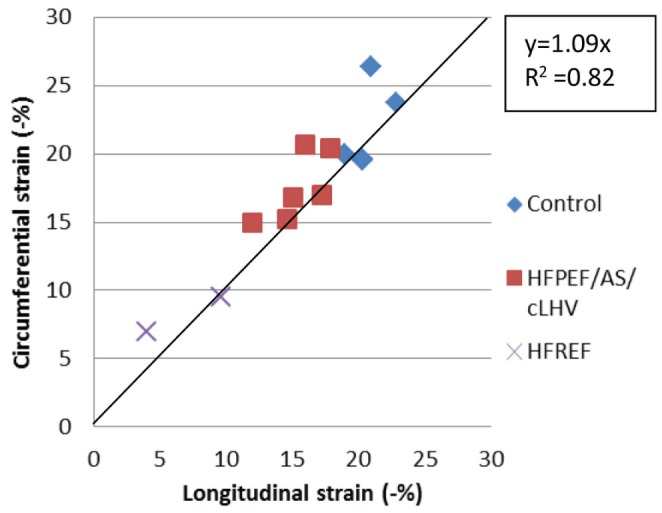
In vivo data have been unable to provide conclusive results with regard to the relative impact of circumferential and longitudinal shortening on stroke volume. The objective of the present study was to assess the relative contribution of circumferential and longitudinal myocardial shortening to left ventricular stroke volume and ejection fraction, and to evaluate the effect of left ventricular hypertrophy. A two-shell, three-dimensional mathematical model was used to assess the individual contributions of longitudinal and midwall circumferential shortening (or strain) to stroke volume and ejection fraction. Reducing either circumferential or longitudinal shortening resulted in a reduced ejection fraction and stroke volume. The stroke volume fell by 43% when circumferential strain was reduced from -20% to -5%, but only by 19% when longitudinal strain was similarly reduced. The sole contribution of circumferential and longitudinal shortening to stroke volume was 67% and 33%, respectively. These proportions were independent of wall thickness. The present study demonstrated that both longitudinal and midwall circumferential shortening contribute to different extents depending on the degree of abnormality of myocardial shortening. Contrary to most previous studies, the present study shows that circumferential shortening has a relatively greater contribution to stroke volume (ie, two-thirds) and ejection fraction than longitudinal shortening. These observations have important clinical and research implications in the assessment of left ventricular function.
Keywords: Ejection fraction; Mathematical modelling; Myocardial mechanics; Myocardial strain; Stroke volume.
Figures
Similar articles
-
Relation of left ventricular longitudinal and circumferential shortening to ejection fraction in the presence or in the absence of mild hypertension.J Hypertens. 1997 Sep;15(9):1011-7. doi: 10.1097/00004872-199715090-00012. J Hypertens. 1997. PMID: 9321749
-
Geometric changes allow normal ejection fraction despite depressed myocardial shortening in hypertensive left ventricular hypertrophy.J Am Coll Cardiol. 1995 Jul;26(1):195-202. doi: 10.1016/0735-1097(95)00153-q. J Am Coll Cardiol. 1995. PMID: 7797752
-
Combined Circumferential and Longitudinal Left Ventricular Systolic Dysfunction in Patients with Rheumatoid Arthritis without Overt Cardiac Disease.J Am Soc Echocardiogr. 2016 Jul;29(7):689-98. doi: 10.1016/j.echo.2016.01.004. Epub 2016 Feb 24. J Am Soc Echocardiogr. 2016. PMID: 26922258
-
Reduced left ventricular systolic pump performance and depressed myocardial contractile function in patients > 65 years of age with normal ejection fraction and a high relative wall thickness.Am J Cardiol. 1995 Oct 1;76(10):702-5. doi: 10.1016/s0002-9149(99)80201-x. Am J Cardiol. 1995. PMID: 7572629 Clinical Trial.
-
Rationale of echocardiographic assessment of left ventricular wall stress and midwall mechanics in hypertensive heart disease.Eur J Echocardiogr. 2002 Sep;3(3):192-8. doi: 10.1053/euje.2002.0163. Eur J Echocardiogr. 2002. PMID: 12144838 Review.
Cited by
-
Global longitudinal active strain energy density (GLASED): age and sex differences between young and veteran athletes.Echo Res Pract. 2024 Jul 15;11(1):17. doi: 10.1186/s44156-024-00052-1. Echo Res Pract. 2024. PMID: 39004742 Free PMC article.
-
Embedded Computational Heart Model for External Ventricular Assist Device Investigations.Cardiovasc Eng Technol. 2022 Oct;13(5):764-782. doi: 10.1007/s13239-022-00610-w. Epub 2022 Mar 15. Cardiovasc Eng Technol. 2022. PMID: 35292915 Free PMC article.
-
Quantification of Myocardial Contraction Fraction with Three-Dimensional Automated, Machine-Learning-Based Left-Heart-Chamber Metrics: Diagnostic Utility in Hypertrophic Phenotypes and Normal Ejection Fraction.J Clin Med. 2023 Aug 25;12(17):5525. doi: 10.3390/jcm12175525. J Clin Med. 2023. PMID: 37685592 Free PMC article.
-
Left ventricular longitudinal shortening: relation to stroke volume and ejection fraction in ageing, blood pressure, body size and gender in the HUNT3 study.Open Heart. 2020 Sep;7(2):e001243. doi: 10.1136/openhrt-2020-001243. Open Heart. 2020. PMID: 32978265 Free PMC article.
-
Association Between Left Ventricular Mechanical Deformation and Myocardial Fibrosis in Nonischemic Cardiomyopathy.J Am Heart Assoc. 2020 Oct 20;9(19):e016797. doi: 10.1161/JAHA.120.016797. Epub 2020 Oct 2. J Am Heart Assoc. 2020. PMID: 33006296 Free PMC article.
References
-
- MacIver DH. A mathematical model of left ventricular contraction and its application in heart disease. In: Atherton M, Collins M, Dayer M, editors. Repair and redesign of physiological systems. Boston: WIT Press; 2008. pp. 65–86.
-
- MacIver DH. Current controversies in heart failure with a preserved ejection fraction. Fut Cardiol. 2010;6:97–111. - PubMed
-
- Anderson RH, Ho SY, Redmann K, Sanchez-Quintana D, Lunkenheimer PP. The anatomical arrangement of the myocardial cells making up the ventricular mass. Eur J Cardiothorac Surg. 2005;28:517–25. - PubMed
-
- MacIver DH. Understanding myocardial deformation, ‘global systolic function’ and abnormal geometry. Heart. 2009. eletter:Re: - DOI
-
- MacIver DH. A new method for quantification of left ventricular systolic function using a corrected ejection fraction. Eur J Echocardiog. 2011;12:228–34. - PubMed
LinkOut - more resources
Full Text Sources