

doi: 10.1055/s-0031-1293517.
The use of a Kirschner wire in the treatment of a comminuted le fort I fracture: a case report
Affiliations
- PMID: 23205174
- PMCID: PMC3314255
- DOI: 10.1055/s-0031-1293517
Item in Clipboard
The use of a Kirschner wire in the treatment of a comminuted le fort I fracture: a case report
Craniomaxillofac Trauma Reconstr.
2011 Dec.
Abstract
Simultaneous fracture of the maxilla and cervical vertebrae rarely occurs in bicycling accidents. The following case report describes a simple technique for closed reduction of a severely comminuted maxillary fracture with shattering of the dentoalveolar process. The combination of a rigid external distractor halo frame on the skull, a Kirschner wire through the maxilla, and an intermaxillary wire fixation resulted in stable vertical and sagittal correction of the fragmented maxilla with adequate access and minimal manipulation and without necessitating removal of the cervical collar.
Keywords: Kirschner wire; Le Fort I fracture; RED halo frame.
Figures

Preoperative computed tomography 3-D reconstruction (A), axial view (B), and coronal view (C) showing comminuted Le Fort I fracture.

Sagittal (A) and anteroposterior (B) illustration of the Kirschner wire position.

Perioperative images (A to D) of the Kirschner wire and rigid external distractor frame in place.
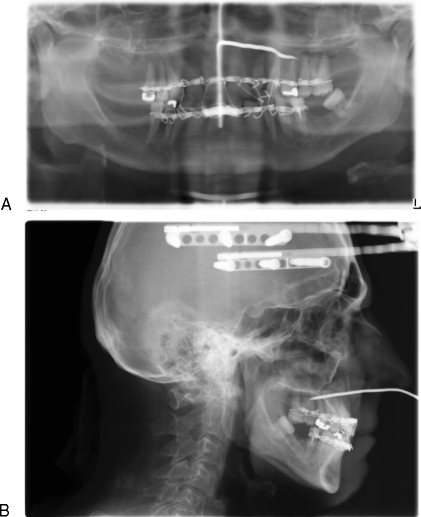
Panoramic radiograph (A) and lateral cephalometric radiograph (B) 6 days postoperative.

Clinical photographs of the patient 1 year after treatment with normal range of opening (A) and normal occlusion (B).

Clinical photograph of the patient before (A) and 1 year after (B) treatment. A cone beam computed tomography 1 year after treatment to document bone healing in axial view (C), coronal view (D), and sagittal view (E).
Similar articles
-
[Clinical effects of Kirschner wire with hole transverse fixation combined with titanium cable purse string suture for the treatment of refractory fracture of patellar comminuted fracture].Zhongguo Gu Shang. 2018 Oct 25;31(10):894-898. doi: 10.3969/j.issn.1003-0034.2018.10.003. Zhongguo Gu Shang. 2018. PMID: 30373339 Chinese.
-
Stability of the Le Fort I osteotomy with anterior internal fixation alone: a case series.J Oral Maxillofac Surg. 2005 May;63(5):629-34. doi: 10.1016/j.joms.2004.12.013. J Oral Maxillofac Surg. 2005. PMID: 15883936
-
Inferior positioning of the maxilla by a Le Fort I osteotomy: a review of 25 patients with vertical maxillary deficiency.J Craniomaxillofac Surg. 1996 Apr;24(2):69-77. doi: 10.1016/s1010-5182(96)80015-1. J Craniomaxillofac Surg. 1996. PMID: 8773886
-
Long-term skeletal stability after maxillary advancement with distraction osteogenesis using a rigid external distraction device in cleft maxillary deformities.Plast Reconstr Surg. 2004 Nov;114(6):1382-92; discussion 1393-4. doi: 10.1097/01.prs.0000138593.89303.1b. Plast Reconstr Surg. 2004. PMID: 15509923 Review.
-
Blindness as a complication of Le Fort I osteotomy for maxillary distraction.Plast Reconstr Surg. 2002 Feb;109(2):688-98; discussion 699-700. doi: 10.1097/00006534-200202000-00041. Plast Reconstr Surg. 2002. PMID: 11818854 Review.
References
-
- Gassner R, Tuli T, Emshoff R, Waldhart E. Mountainbiking—a dangerous sport: comparison with bicycling on oral and maxillofacial trauma. Int J Oral Maxillofac Surg. 1999;28:188–191. - PubMed
-
- Elahi M ME, Brar M S, Ahmed N, Howley D B, Nishtar S, Mahoney J L. Cervical spine injury in association with craniomaxillofacial fractures. Plast Reconstr Surg. 2008;121:201–208. - PubMed
-
- Haug R H, Prather J, Indresano A T. An epidemiologic survey of facial fractures and concomitant injuries. J Oral Maxillofac Surg. 1990;48:926–932. - PubMed
-
- Mulligan R P, Mahabir R C. The prevalence of cervical spine injury, head injury, or both with isolated and multiple craniomaxillofacial fractures. Plast Reconstr Surg. 2010;126:1647–1651. - PubMed
-
- Elhammali N, Bremerich A, Rustemeyer J. Demographical and clinical aspects of sports-related maxillofacial and skull base fractures in hospitalized patients. Int J Oral Maxillofac Surg. 2010;39:857–862. - PubMed
LinkOut - more resources
Full Text Sources