

Post-transplantation cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation
- PMID: 23206845
- PMCID: PMC3808078
- DOI: 10.1053/j.seminoncol.2012.09.005
Post-transplantation cyclophosphamide for tolerance induction in HLA-haploidentical bone marrow transplantation
Abstract
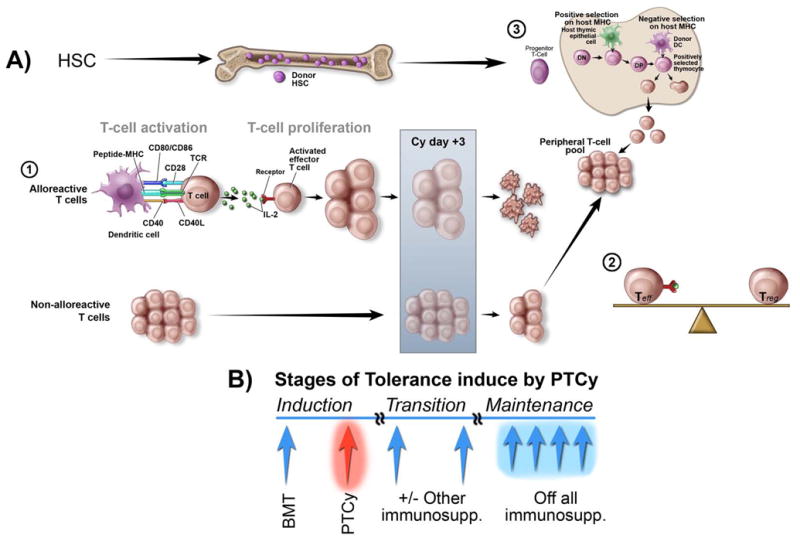
Allogeneic hematopoietic stem cell transplantation (alloSCT) is a potentially curative therapy for many hematologic and immunologic diseases. Further, partial or full donor hematopoietic chimerism following alloSCT may be sufficient to guarantee immunologic tolerance to solid organs from the same donor, obviating any requirement for prolonged pharmacologic immunosuppression. Despite alloSCT's potential, the procedure is beset by two major limitations. The first relates to the procedure's toxicity, including conditioning regimen toxicity, graft-versus-host disease (GVHD), and infection. The second limitation is the lack of histocompatible donors. A human leukocyte antigen (HLA)-matched sibling or unrelated donor cannot be identified expeditiously for up to 40% of patients. Historically, alloSCT from partially HLA-mismatched, or HLA-haploidentical, relatives has been complicated by unacceptably high incidences of graft rejection, severe GVHD, and non-relapse mortality. Recently, our groups have developed a method to selectively deplete alloreactive cells in vivo by administering high doses of cyclophosphamide in a narrow window after transplantation. Using high-dose, post-transplantation cyclophosphamide (PT/Cy), crossing the HLA barrier in alloSCT is now feasible and donors can be found for nearly all patients. This review discusses the history of HLA-haploidentical SCT, recent clinical results, and immunologic mechanisms of action of high-dose PT/Cy for prevention of graft rejection and GVHD.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- Beatty PG, Clift RA, Mickelson EM, et al. Marrow transplantation from related donors other than HLA-identical siblings. N Engl J Med. 1985;313:765–71. - PubMed
-
- Buckner CD, Epstein RB, Rudolph RH, Clift RA, Storb R, Thomas ED. Allogeneic marrow engraftment following whole body irradiation in a patient with leukemia. Blood. 1970;35:741–50. - PubMed
-
- Clift RA, Hansen JA, Thomas ED, et al. Marrow transplantation from donors other than HLA-identical siblings. Transplantation. 1979;28:235–42. - PubMed
-
- Powles RL, Morgenstern GR, Kay HE, et al. Mismatched family donors for bone-marrow transplantation as treatment for acute leukaemia. Lancet. 1983;1:612–5. - PubMed
-
- Spitzer TR. Engraftment syndrome following hematopoietic stem cell transplantation. Bone Marrow Transplant. 2001;27:893–8. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
