

Bench-to-bedside review: Clinical experience with the endotoxin activity assay
- PMID: 23206992
- PMCID: PMC3672550
- DOI: 10.1186/cc11495
Bench-to-bedside review: Clinical experience with the endotoxin activity assay
Abstract
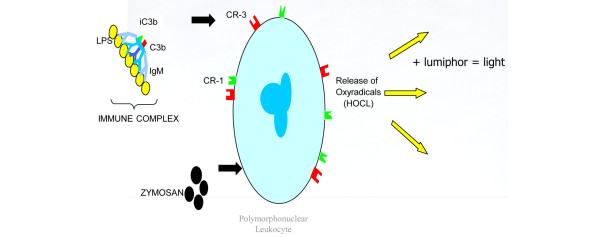
Endotoxin detection in human patients has been a difficult challenge, in part due to the fact that the conserved active portion of the molecule (lipid A) is a relatively small epitope only amenable to binding by a single ligand at any one instance and low levels (pg/ml) are capable of stimulating the immune system. The endotoxin activity assay, a bioassay based on neutrophil activation by complement opsonized immune complexes of lipopolysaccharide (LPS), has allowed the specific detection of the lipid A epitope of LPS in a rapid whole blood assay format. This review summarizes diagnostic studies utilizing the endotoxin activity assay in a variety of hospital patient populations in whom endotoxin is postulated to play a significant role in disease etiology. These include ICU patients at risk of developing 'sepsis syndrome', abdominal and cardiovascular surgery patients and patients with serious traumatic injury. Significant features of these studies include the high negative predictive value of the assay (98.6%) for rule out of Gram-negative infection, ability to risk stratify patients progressing to severe sepsis (odds ratio 3.0) and evidence of LPS release in patients with gut hypoperfusion. Preliminary studies have successfully combined the assay with anti-LPS removal strategies to prospectively identify patients who might benefit from this therapy with early evidence of clinical benefit.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
