

Epidemiology and risk factors for gastroesophageal junction tumors: understanding the rising incidence of this disease
- PMID: 23207041
- PMCID: PMC3535292
- DOI: 10.1016/j.semradonc.2012.09.008
Epidemiology and risk factors for gastroesophageal junction tumors: understanding the rising incidence of this disease
Abstract
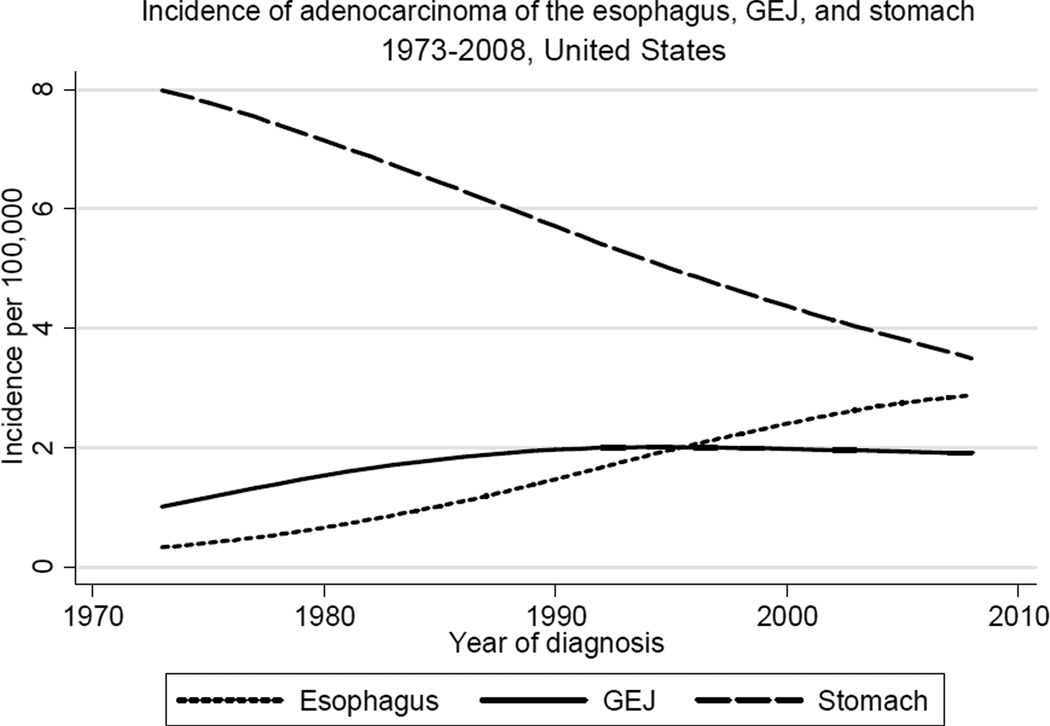
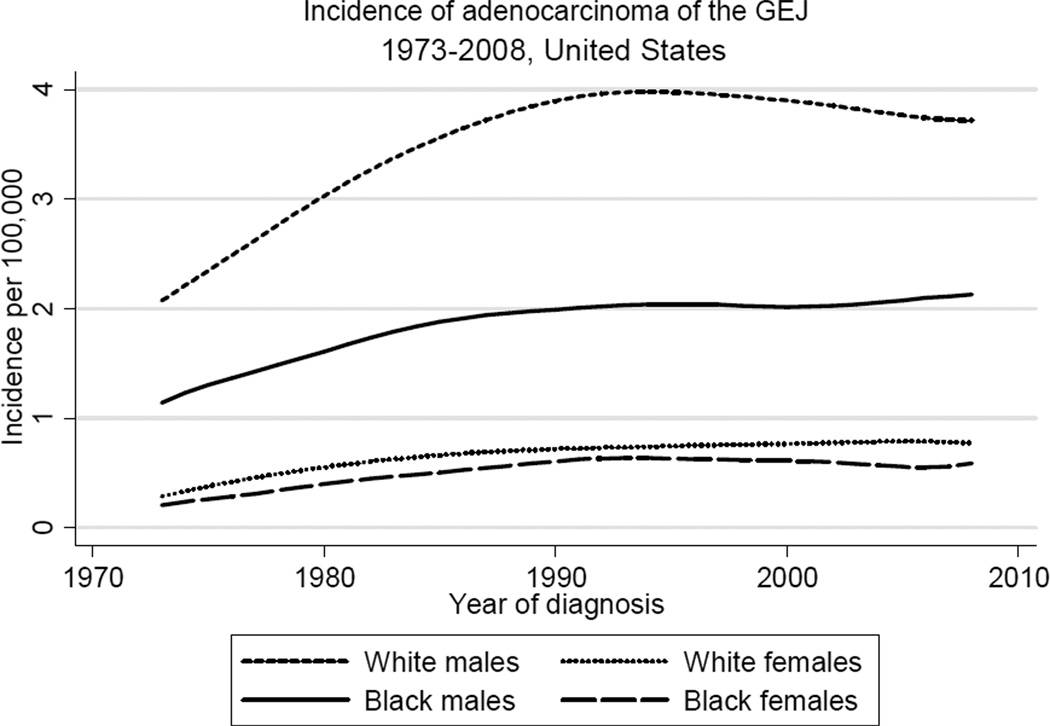
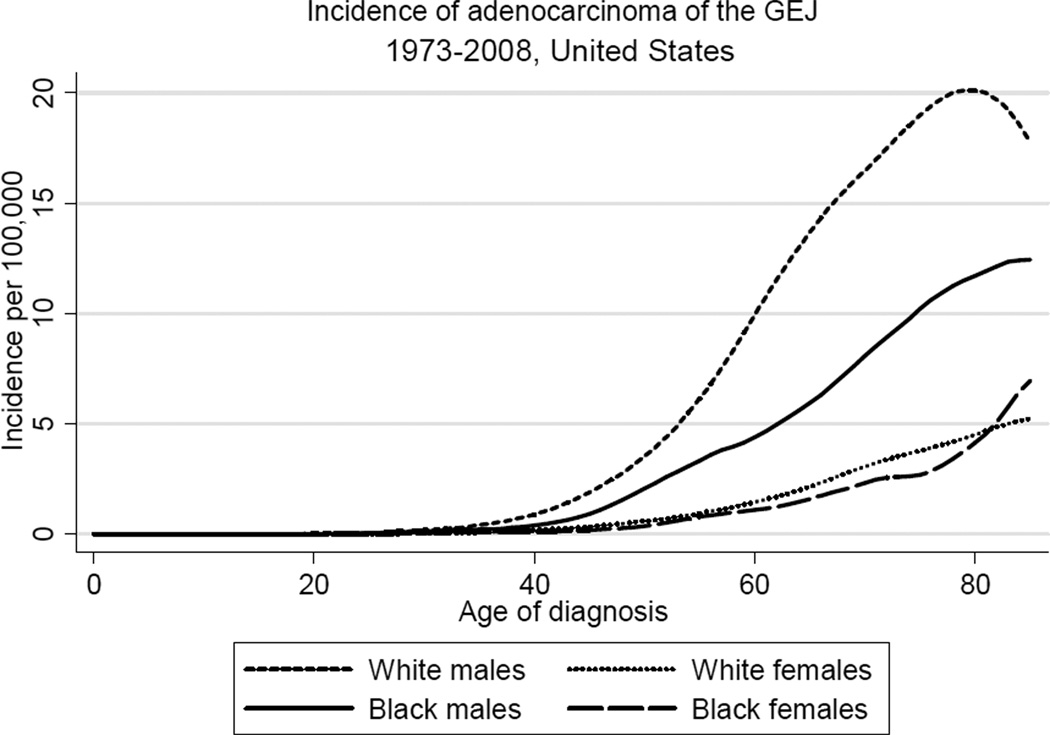
Gastroesophageal (GE) junction carcinoma is a rare but often lethal condition with increasing importance as a public health problem in recent decades. Whereas diagnosis of this disease has been complicated historically by the lack of uniform classification standards, available data from the Surveillance, Epidemiology, and End Results cancer registry program in the United States show an approximate 2.5-fold increase in the incidence of GE junction adenocarcinoma from 1973 to 1992, with rates stabilizing in the past 2 decades. Similar proportional trends are observed among subgroups defined by race and gender, but rates are significantly higher in males relative to females, and in white males relative to black males. Smoking, obesity, and GE reflux disease are significant risk factors for GE junction adenocarcinoma, and may account for a substantial fraction of total disease burden. Infection with Helicobacter pylori has been associated with reduced incidence, and high dietary fiber intake has also been linked to lower disease risk. Ongoing studies continue to explore a potential role for nonsteroidal anti-inflammatory drugs in chemoprevention.
Copyright © 2013 Elsevier Inc. All rights reserved.
Figures

References
-
- Rusch VW. Are cancers of the esophagus, gastroesophageal junction, and cardia one disease, two, or several? Semin Oncol. 2004;31(4):444–449. - PubMed
-
- Siewert JR, Stein HJ. Classification of adenocarcinoma of the oesophagogastric junction. Br J Surg. 1998;85(11):1457–1459. - PubMed
-
- Blot WJ, Devesa SS, Kneller RW, Fraumeni JF., Jr Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991;265(10):1287–1289. - PubMed
-
- Botterweck AA, Schouten LJ, Volovics A, Dorant E, van Den Brandt PA. Trends in incidence of adenocarcinoma of the oesophagus and gastric cardia in ten European countries. Int J Epidemiol. 2000;29(4):645–654. - PubMed
-
- Hansson LE, Sparen P, Nyren O. Increasing incidence of carcinoma of the gastric cardia in Sweden from 1970 to 1985. Br J Surg. 1993;80(3):374–377. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
