

In vivo bioluminescence imaging to evaluate systemic and topical antibiotics against community-acquired methicillin-resistant Staphylococcus aureus-infected skin wounds in mice
- PMID: 23208713
- PMCID: PMC3553733
- DOI: 10.1128/AAC.01003-12
In vivo bioluminescence imaging to evaluate systemic and topical antibiotics against community-acquired methicillin-resistant Staphylococcus aureus-infected skin wounds in mice
Abstract
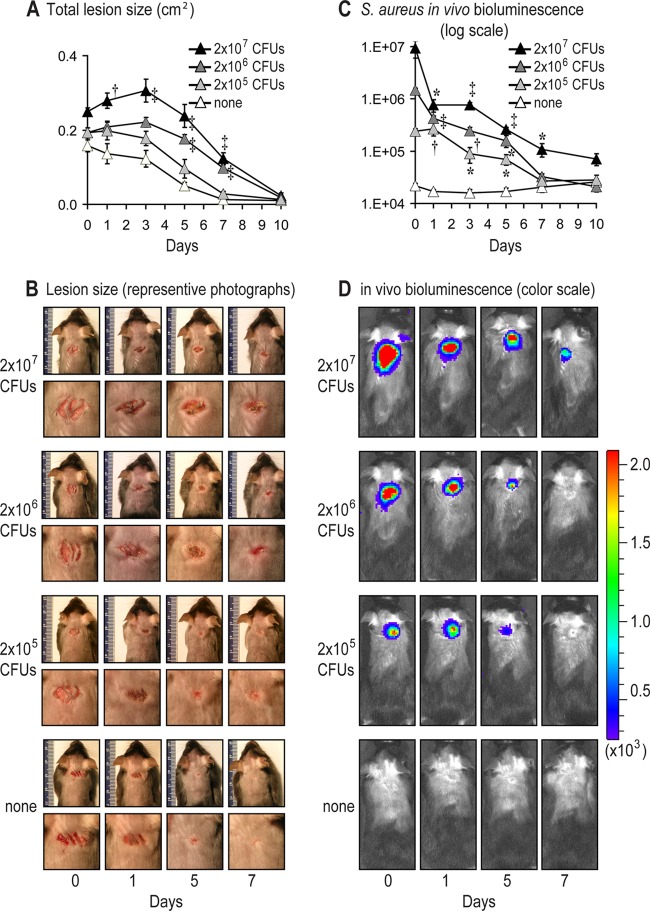
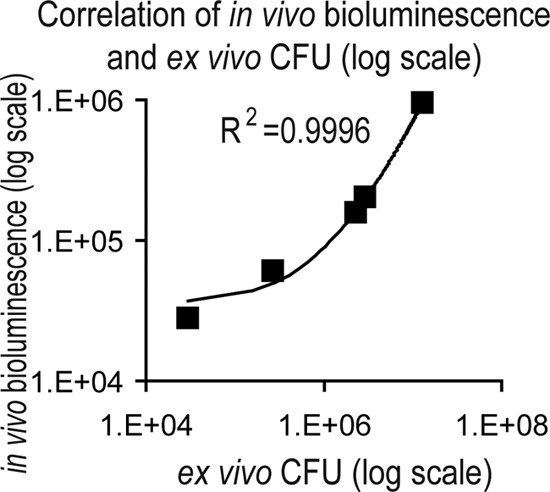
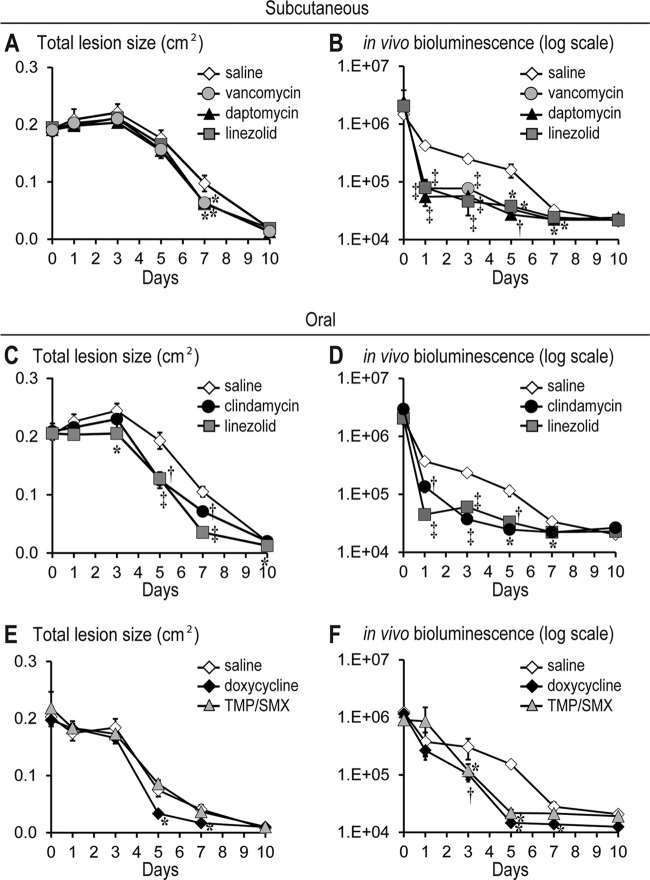
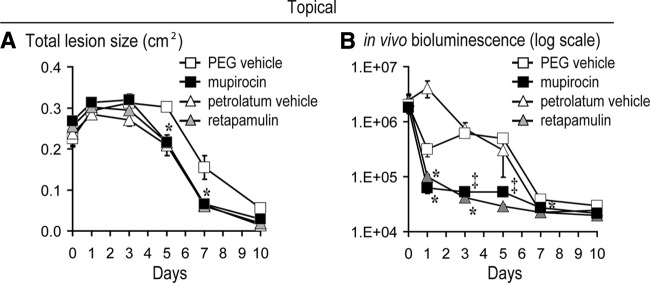
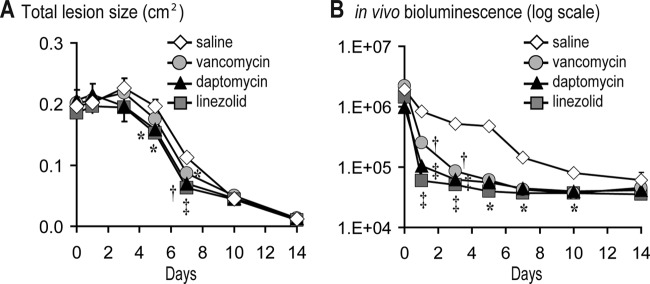
Community-acquired methicillin-resistant Staphylococcus aureus (CA-MRSA) frequently causes skin and soft tissue infections, including impetigo, cellulitis, folliculitis, and infected wounds and ulcers. Uncomplicated CA-MRSA skin infections are typically managed in an outpatient setting with oral and topical antibiotics and/or incision and drainage, whereas complicated skin infections often require hospitalization, intravenous antibiotics, and sometimes surgery. The aim of this study was to develop a mouse model of CA-MRSA wound infection to compare the efficacy of commonly used systemic and topical antibiotics. A bioluminescent USA300 CA-MRSA strain was inoculated into full-thickness scalpel wounds on the backs of mice and digital photography/image analysis and in vivo bioluminescence imaging were used to measure wound healing and the bacterial burden. Subcutaneous vancomycin, daptomycin, and linezolid similarly reduced the lesion sizes and bacterial burden. Oral linezolid, clindamycin, and doxycycline all decreased the lesion sizes and bacterial burden. Oral trimethoprim-sulfamethoxazole decreased the bacterial burden but did not decrease the lesion size. Topical mupirocin and retapamulin ointments both reduced the bacterial burden. However, the petrolatum vehicle ointment for retapamulin, but not the polyethylene glycol vehicle ointment for mupirocin, promoted wound healing and initially increased the bacterial burden. Finally, in type 2 diabetic mice, subcutaneous linezolid and daptomycin had the most rapid therapeutic effect compared with vancomycin. Taken together, this mouse model of CA-MRSA wound infection, which utilizes in vivo bioluminescence imaging to monitor the bacterial burden, represents an alternative method to evaluate the preclinical in vivo efficacy of systemic and topical antimicrobial agents.
Figures
References
-
- Hersh AL, Chambers HF, Maselli JH, Gonzales R. 2008. National trends in ambulatory visits and antibiotic prescribing for skin and soft-tissue infections. Arch. Intern. Med. 168:1585–1591 - PubMed
-
- Moran GJ, Krishnadasan A, Gorwitz RJ, Fosheim GE, McDougal LK, Carey RB, Talan DA. 2006. Methicillin-resistant S. aureus infections among patients in the emergency department. N. Engl. J. Med. 355:666–674 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
