

Neuroimaging in mitochondrial disorders
- PMID: 23208728
- PMCID: PMC3625392
- DOI: 10.1007/s13311-012-0161-6
Neuroimaging in mitochondrial disorders
Abstract
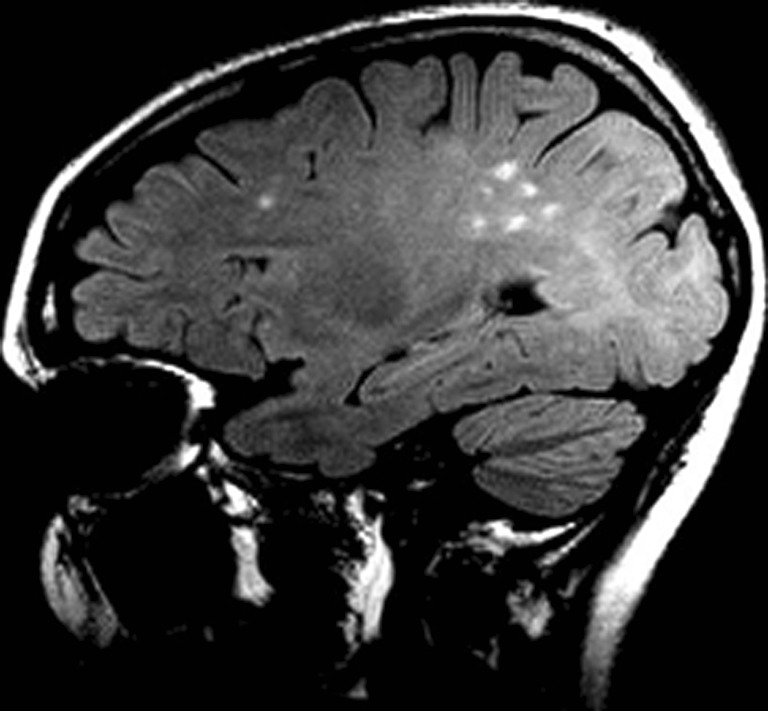
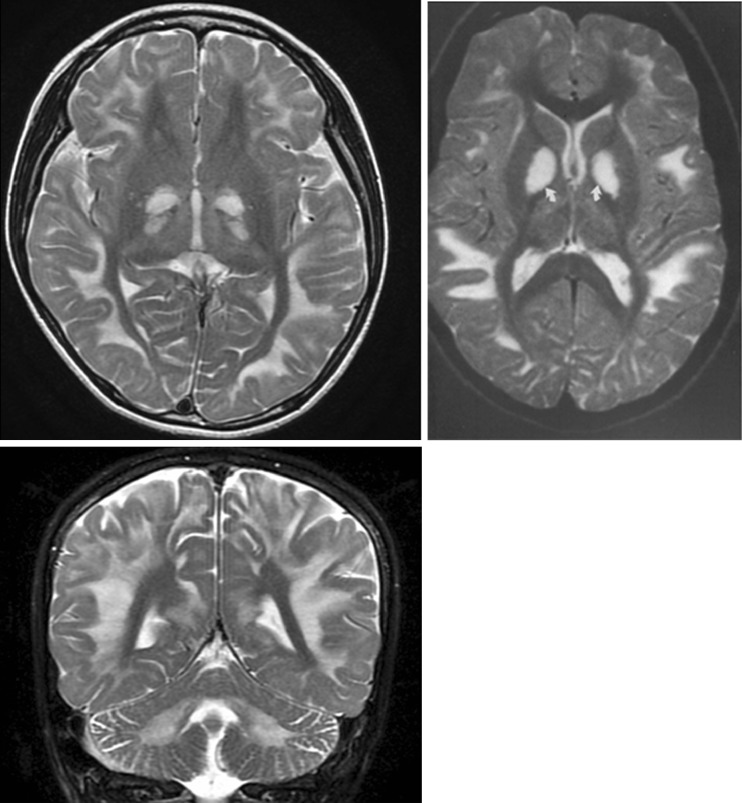
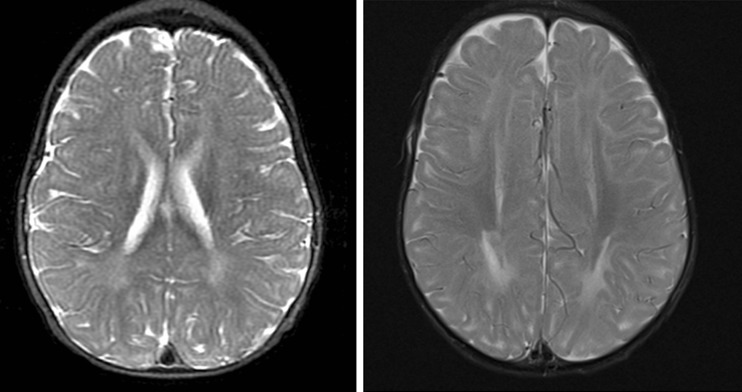
Mutations in either nuclear DNA or mitochondrial DNA can result in disruption of oxidative phosphorylation and lead to mitochondrial dysfunction. Mitochondrial disease manifestations occur predominantly in the central nervous system, peripheral nervous system, and/or involve several organ systems. The consequences range from manifestations of a single organ or tissues, such as muscle fatigue, if confined only to muscle, seizures, intellectual disabilities, dementia, and stroke (if to the central nervous system), leading to disability or even early death. The definitive diagnosis of a mitochondrial disorder can be difficult to establish. Criteria and checklists have been established and are more reflective of adult disease. However, in children, when symptoms suggest a mitochondrial disease, neuroimaging features may have more diagnostic impact and additionally these can be used to follow the course, evolution, and recovery of the disease. This review will demonstrate the common neuroimaging patterns in patients with mitochondrial disorders and point out how various newer neuroimaging modalities may be exploited to glean information as to the different aspects of mitochondrial dysfunction or resulting neurological and cognitive disruption, although reports in the literature using these methods remain sparse.
Figures



References
-
- DiMauro S. Mitochondrial medicine. Biochim Biophys Acta. 2004;1658:107–114. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
