

Screening and rapid molecular diagnosis of tuberculosis in prisons in Russia and Eastern Europe: a cost-effectiveness analysis
- PMID: 23209384
- PMCID: PMC3507963
- DOI: 10.1371/journal.pmed.1001348
Screening and rapid molecular diagnosis of tuberculosis in prisons in Russia and Eastern Europe: a cost-effectiveness analysis
Abstract
Background: Prisons of the former Soviet Union (FSU) have high rates of multidrug-resistant tuberculosis (MDR-TB) and are thought to drive general population tuberculosis (TB) epidemics. Effective prison case detection, though employing more expensive technologies, may reduce long-term treatment costs and slow MDR-TB transmission.
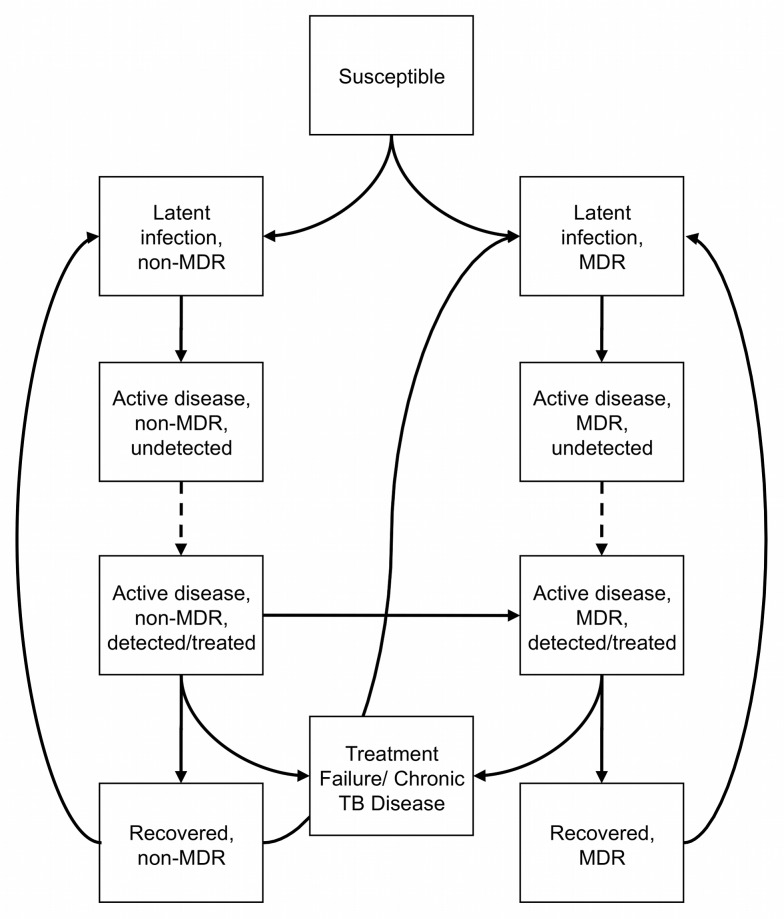
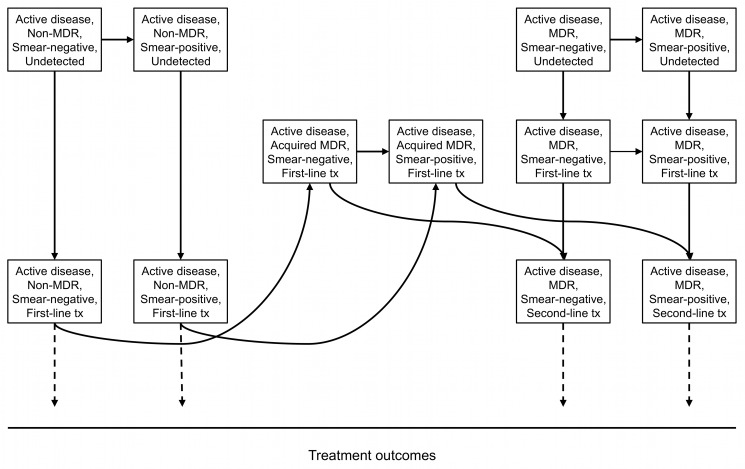
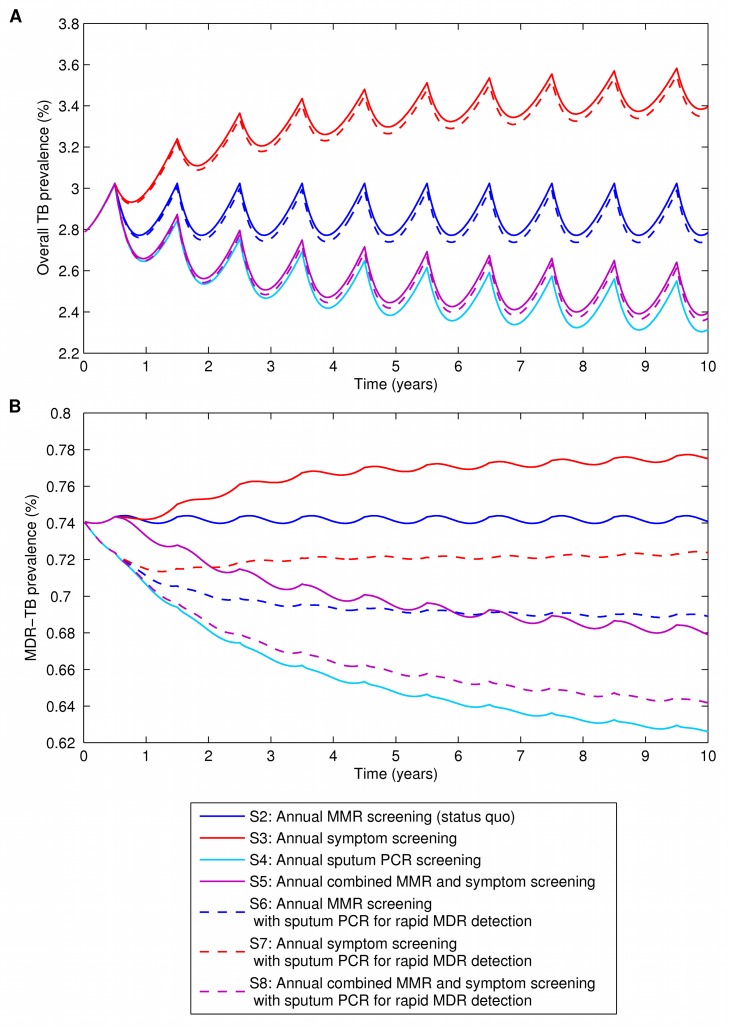
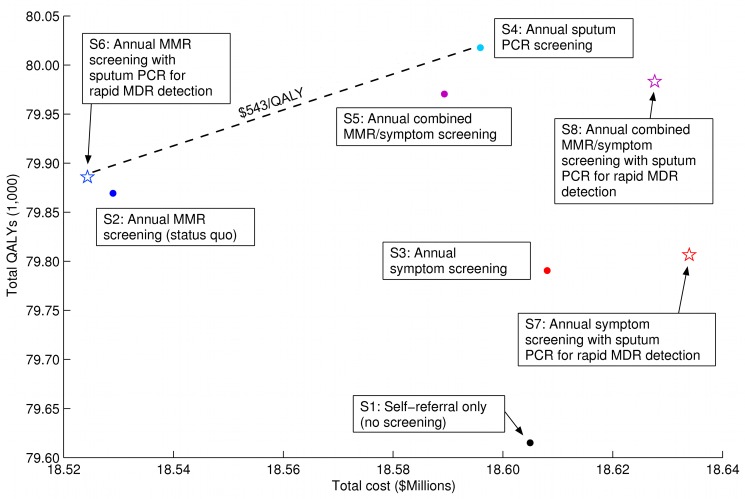
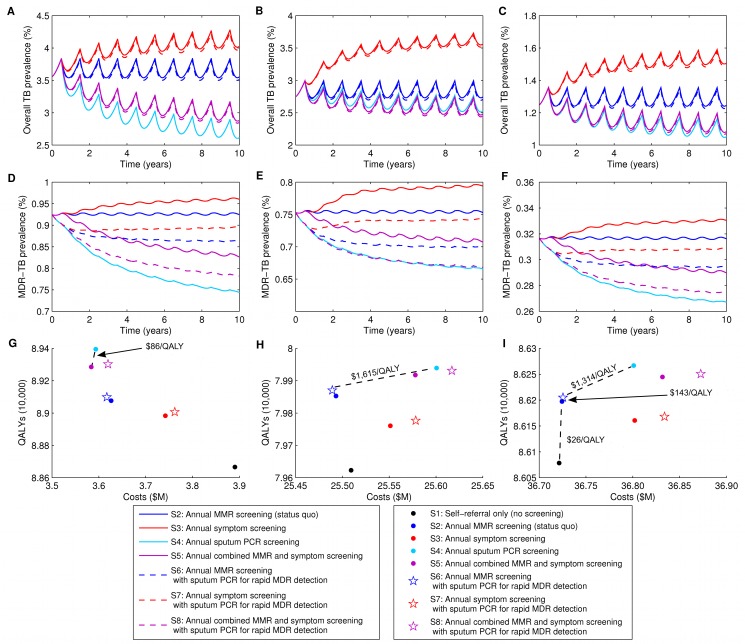
Methods and findings: We developed a dynamic transmission model of TB and drug resistance matched to the epidemiology and costs in FSU prisons. We evaluated eight strategies for TB screening and diagnosis involving, alone or in combination, self-referral, symptom screening, mass miniature radiography (MMR), and sputum PCR with probes for rifampin resistance (Xpert MTB/RIF). Over a 10-y horizon, we projected costs, quality-adjusted life years (QALYs), and TB and MDR-TB prevalence. Using sputum PCR as an annual primary screening tool among the general prison population most effectively reduced overall TB prevalence (from 2.78% to 2.31%) and MDR-TB prevalence (from 0.74% to 0.63%), and cost US$543/QALY for additional QALYs gained compared to MMR screening with sputum PCR reserved for rapid detection of MDR-TB. Adding sputum PCR to the currently used strategy of annual MMR screening was cost-saving over 10 y compared to MMR screening alone, but produced only a modest reduction in MDR-TB prevalence (from 0.74% to 0.69%) and had minimal effect on overall TB prevalence (from 2.78% to 2.74%). Strategies based on symptom screening alone were less effective and more expensive than MMR-based strategies. Study limitations included scarce primary TB time-series data in FSU prisons and uncertainties regarding screening test characteristics.
Conclusions: In prisons of the FSU, annual screening of the general inmate population with sputum PCR most effectively reduces TB and MDR-TB prevalence, doing so cost-effectively. If this approach is not feasible, the current strategy of annual MMR is both more effective and less expensive than strategies using self-referral or symptom screening alone, and the addition of sputum PCR for rapid MDR-TB detection may be cost-saving over time.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Population health impact and cost-effectiveness of tuberculosis diagnosis with Xpert MTB/RIF: a dynamic simulation and economic evaluation.PLoS Med. 2012;9(11):e1001347. doi: 10.1371/journal.pmed.1001347. Epub 2012 Nov 20. PLoS Med. 2012. PMID: 23185139 Free PMC article.
-
Cost-benefit analysis of Xpert MTB/RIF for tuberculosis suspects in German hospitals.Eur Respir J. 2016 Feb;47(2):575-87. doi: 10.1183/13993003.01333-2015. Epub 2015 Dec 2. Eur Respir J. 2016. PMID: 26647440
-
A cost-benefit algorithm for rapid diagnosis of tuberculosis and rifampicin resistance detection during mass screening campaigns.BMC Infect Dis. 2022 Mar 4;22(1):219. doi: 10.1186/s12879-022-07157-0. BMC Infect Dis. 2022. PMID: 35246071 Free PMC article.
-
Tuberculosis active case-finding interventions and approaches for prisoners in sub-Saharan Africa: a systematic scoping review.BMC Infect Dis. 2020 Aug 5;20(1):570. doi: 10.1186/s12879-020-05283-1. BMC Infect Dis. 2020. PMID: 32758165 Free PMC article.
-
A model of tuberculosis screening for pregnant women in resource-limited settings using Xpert MTB/RIF.J Pregnancy. 2012;2012:565049. doi: 10.1155/2012/565049. Epub 2011 Oct 5. J Pregnancy. 2012. PMID: 22007302 Free PMC article. Review.
Cited by
-
Diagnostic accuracy of active pulmonary tuberculosis screening during detention admission: a systematic review.J Med Life. 2024 Jul;17(7):671-681. doi: 10.25122/jml-2024-0155. J Med Life. 2024. PMID: 39440335 Free PMC article.
-
High tuberculosis prevalence in a South African prison: the need for routine tuberculosis screening.PLoS One. 2014 Jan 30;9(1):e87262. doi: 10.1371/journal.pone.0087262. eCollection 2014. PLoS One. 2014. PMID: 24498059 Free PMC article.
-
Comparing the cost-effectiveness of the MPT64-antigen detection test to Xpert MTB/RIF and ZN-microscopy for the diagnosis of Extrapulmonary Tuberculosis: An economic evaluation modelling study.PLOS Glob Public Health. 2024 Aug 8;4(8):e0003414. doi: 10.1371/journal.pgph.0003414. eCollection 2024. PLOS Glob Public Health. 2024. PMID: 39116052 Free PMC article.
-
Cost-effectiveness of improvements in diagnosis and treatment accessibility for tuberculosis control in India.Int J Tuberc Lung Dis. 2015 Sep;19(9):1115-24, i-xv. doi: 10.5588/ijtld.15.0158. Int J Tuberc Lung Dis. 2015. PMID: 26260835 Free PMC article.
-
Optimal timing of drug sensitivity testing for patients on first-line tuberculosis treatment.Health Care Manag Sci. 2018 Dec;21(4):632-646. doi: 10.1007/s10729-017-9416-4. Epub 2017 Aug 31. Health Care Manag Sci. 2018. PMID: 28861650 Free PMC article.
References
-
- World Health Organization (2010) Global tuberculosis control 2010. Geneva: World Health Organization.
-
- Stuckler D, Basu S, McKee M, King L (2008) Mass incarceration can explain population increases in TB and multidrug-resistant TB in European and central Asian countries. Proc Natl Acad Sci U S A 105: 13280–13285 doi:10.1073/pnas.0801200105. - DOI - PMC - PubMed
-
- Dara M, Grzemska M, Kimerling ME, Reyes H, Zagorskiy A (2009) Guidelines for control of tuberculosis in prisons. Washington (District of Columbia): U.S. Agency for International Development.
-
- Bone A, Aerts A, Grzemska M, Kimerling M, Kluge H, et al... (2000) Tuberculosis control in prisons: a manual for programme managers. Geneva: World Health Organization.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
