

Performance of thirteen clinical rules to distinguish bacterial and presumed viral meningitis in Vietnamese children
- PMID: 23209715
- PMCID: PMC3508924
- DOI: 10.1371/journal.pone.0050341
Performance of thirteen clinical rules to distinguish bacterial and presumed viral meningitis in Vietnamese children
Abstract
Background and purpose: Successful outcomes from bacterial meningitis require rapid antibiotic treatment; however, unnecessary treatment of viral meningitis may lead to increased toxicities and expense. Thus, improved diagnostics are required to maximize treatment and minimize side effects and cost. Thirteen clinical decision rules have been reported to identify bacterial from viral meningitis. However, few rules have been tested and compared in a single study, while several rules are yet to be tested by independent researchers or in pediatric populations. Thus, simultaneous test and comparison of these rules are required to enable clinicians to select an optimal diagnostic rule for bacterial meningitis in settings and populations similar to ours.
Methods: A retrospective cross-sectional study was conducted at the Infectious Department of Pediatric Hospital Number 1, Ho Chi Minh City, Vietnam. The performance of the clinical rules was evaluated by area under a receiver operating characteristic curve (ROC-AUC) using the method of DeLong and McNemar test for specificity comparison.
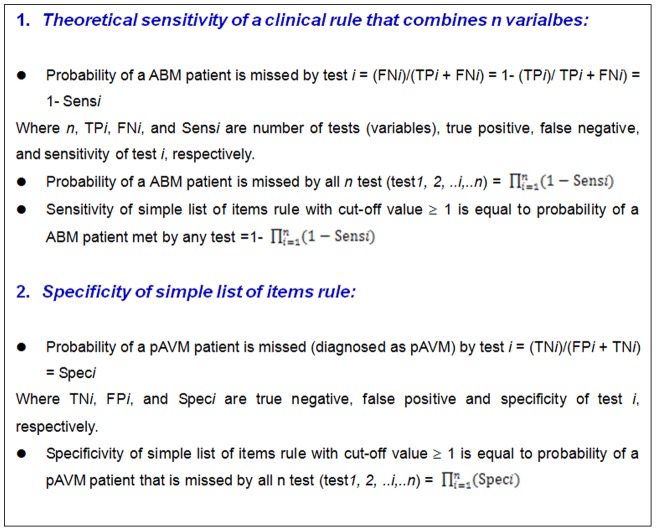
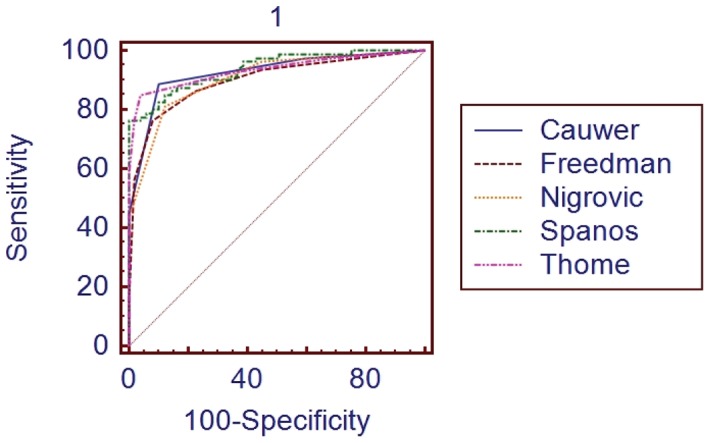
Results: Our study included 129 patients, of whom 80 had bacterial meningitis and 49 had presumed viral meningitis. Spanos's rule had the highest AUC at 0.938 but was not significantly greater than other rules. No rule provided 100% sensitivity with a specificity higher than 50%. Based on our calculation of theoretical sensitivity and specificity, we suggest that a perfect rule requires at least four independent variables that posses both sensitivity and specificity higher than 85-90%.
Conclusions: No clinical decision rules provided an acceptable specificity (>50%) with 100% sensitivity when applying our data set in children. More studies in Vietnam and developing countries are required to develop and/or validate clinical rules and more very good biomarkers are required to develop such a perfect rule.
Conflict of interest statement
Figures
References
-
- Saez-Llorens X, McCracken GH Jr (2003) Bacterial meningitis in children. Lancet 361: 2139–2148. - PubMed
-
- Zimmerli W (2005) How to differentiate bacterial from viral meningitis. Intensive Care Med 31: 1608–1610. - PubMed
-
- Raymond J (2000) [Epidemiology of nosocomial infections in pediatrics]. Pathol Biol (Paris) 48: 879–884. - PubMed
-
- Parasuraman TV, Frenia K, Romero J (2001) Enteroviral meningitis. Cost of illness and considerations for the economic evaluation of potential therapies. Pharmacoeconomics 19: 3–12. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
