

Estimating the global prevalence of inadequate zinc intake from national food balance sheets: effects of methodological assumptions
- PMID: 23209781
- PMCID: PMC3510064
- DOI: 10.1371/journal.pone.0050565
Estimating the global prevalence of inadequate zinc intake from national food balance sheets: effects of methodological assumptions
Abstract
Background: The prevalence of inadequate zinc intake in a population can be estimated by comparing the zinc content of the food supply with the population's theoretical requirement for zinc. However, assumptions regarding the nutrient composition of foods, zinc requirements, and zinc absorption may affect prevalence estimates. These analyses were conducted to: (1) evaluate the effect of varying methodological assumptions on country-specific estimates of the prevalence of dietary zinc inadequacy and (2) generate a model considered to provide the best estimates.
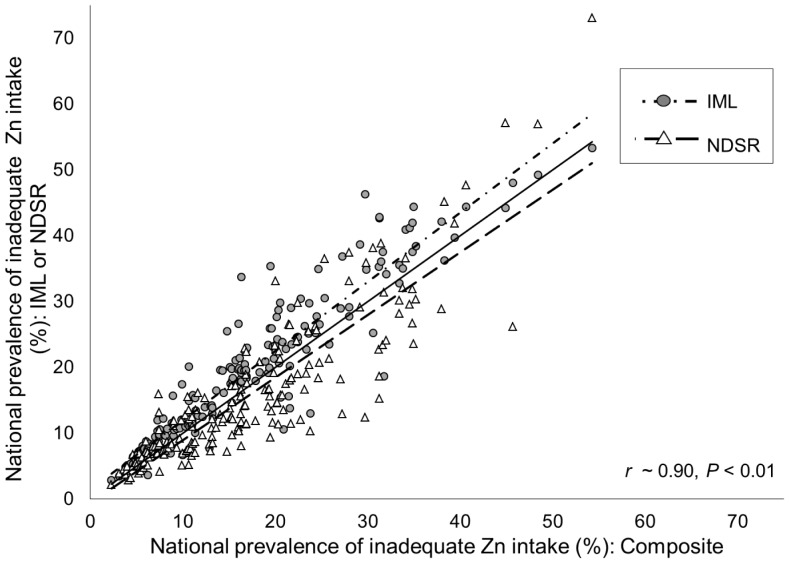
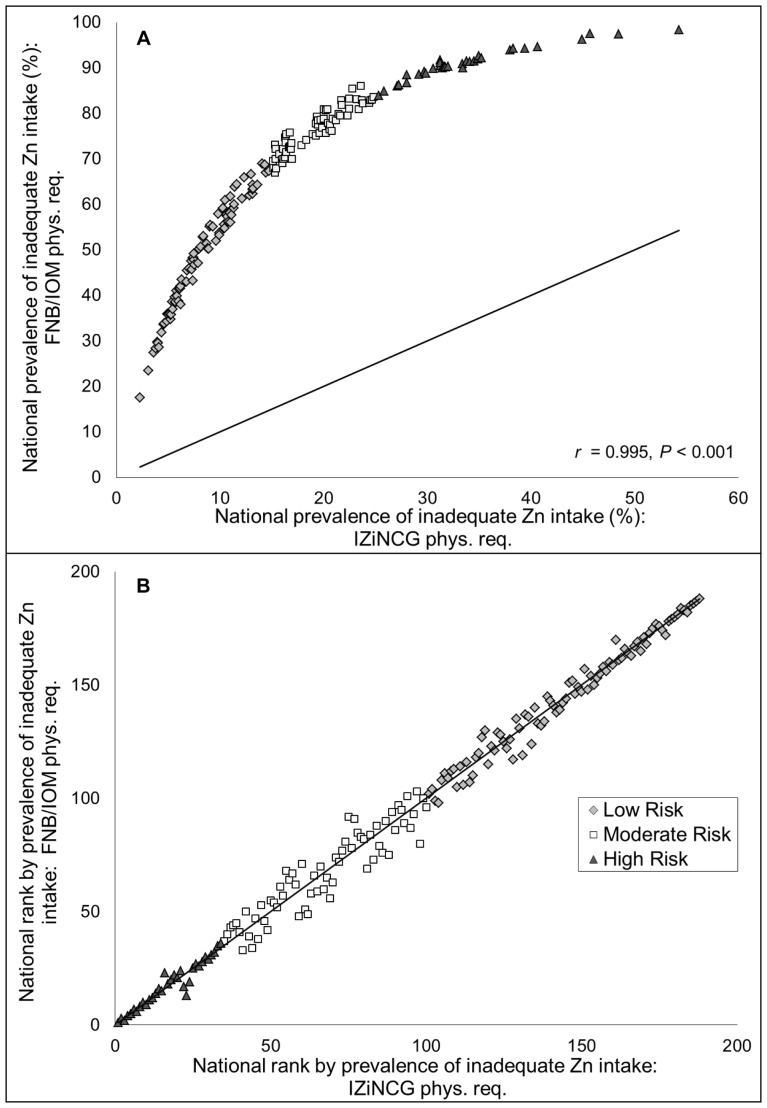
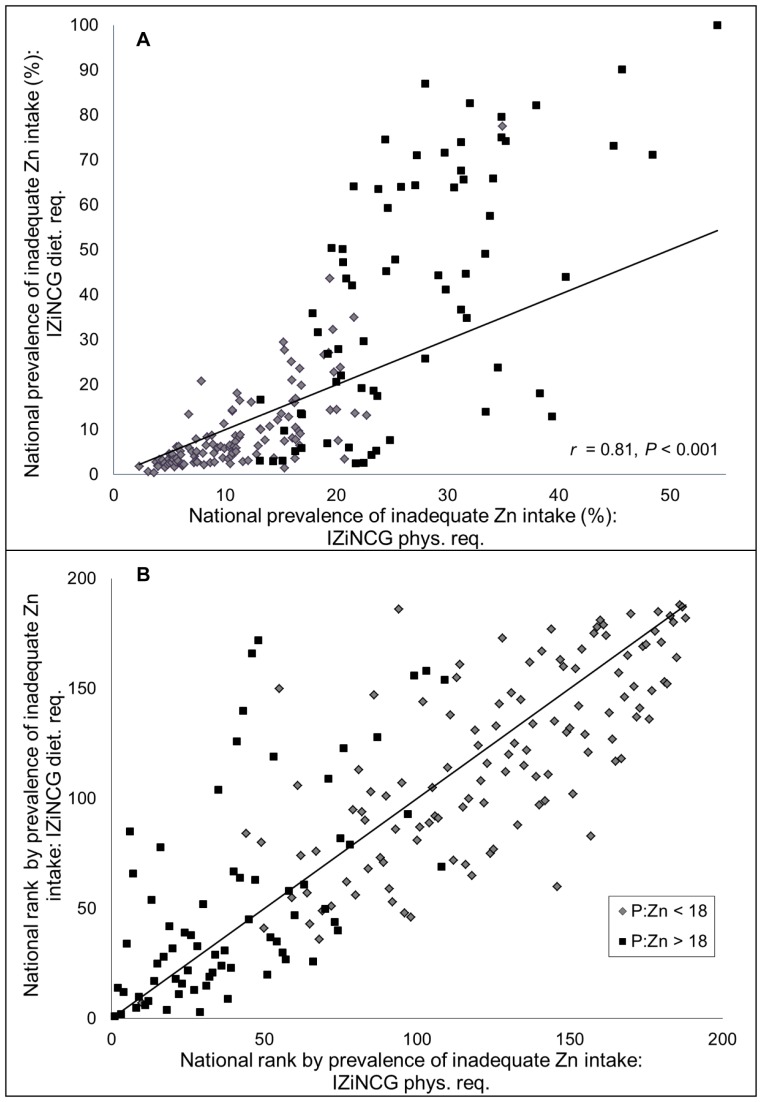
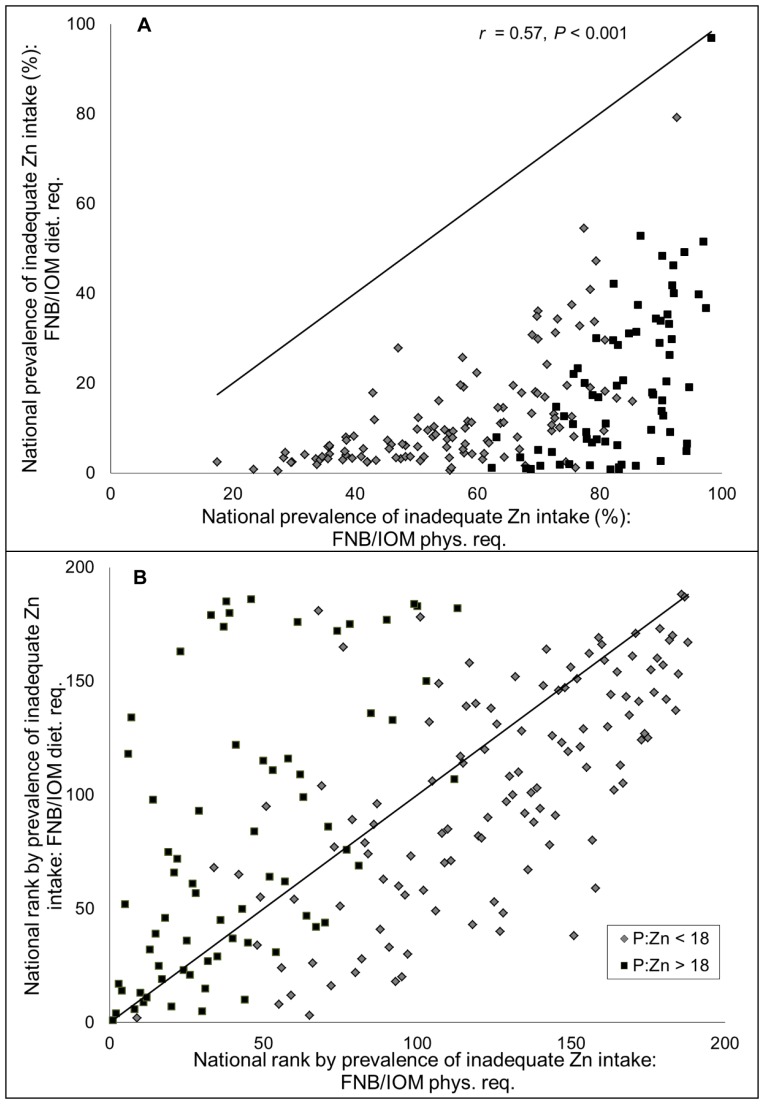
Methodology and principal findings: National food balance data were obtained from the Food and Agriculture Organization of the United Nations. Zinc and phytate contents of these foods were estimated from three nutrient composition databases. Zinc absorption was predicted using a mathematical model (Miller equation). Theoretical mean daily per capita physiological and dietary requirements for zinc were calculated using recommendations from the Food and Nutrition Board of the Institute of Medicine and the International Zinc Nutrition Consultative Group. The estimated global prevalence of inadequate zinc intake varied between 12-66%, depending on which methodological assumptions were applied. However, country-specific rank order of the estimated prevalence of inadequate intake was conserved across all models (r = 0.57-0.99, P<0.01). A "best-estimate" model, comprised of zinc and phytate data from a composite nutrient database and IZiNCG physiological requirements for absorbed zinc, estimated the global prevalence of inadequate zinc intake to be 17.3%.
Conclusions and significance: Given the multiple sources of uncertainty in this method, caution must be taken in the interpretation of the estimated prevalence figures. However, the results of all models indicate that inadequate zinc intake may be fairly common globally. Inferences regarding the relative likelihood of zinc deficiency as a public health problem in different countries can be drawn based on the country-specific rank order of estimated prevalence of inadequate zinc intake.
Conflict of interest statement
Figures
References
-
- Brown KH, Rivera JA, Bhutta Z, Gibson RS, King JC, et al. (2004) International Zinc Nutrition Consultative Group (IZiNCG) technical document #1. Assessment of the risk of zinc deficiency in populations and options for its control. Food Nutr Bull 25: S99–203. - PubMed
-
- de Benoist B, Darnton-Hill I, Davidsson L, Fontaine O (2007) Report of a WHO/UNICEF/IAEA/IZiNCG interagency meeting on zinc status indicators, held in IAEA headquarters, Vienna, December 9, 2005. Food Nutr Bull 28: S399–S484. - PubMed
-
- Gibson RS, Bailey KB, Parnell WR, Wilson N, Ferguson EL (2011) Higher risk of zinc deficiency in New Zealand Pacific school children compared with their Maori and European counterparts: a New Zealand national survey. Br J Nutr 105: 436–446. - PubMed
-
- Ma G, Li Y, Jin Y, Du S, Kok FJ, et al. (2007) Assessment of intake inadequacy and food sources of zinc of people in China. Public Health Nutr 10: 848–854. - PubMed
-
- Villalpando S, Garcia-Guerra A, Ramirez-Silva CI, Mejia-Rodriguez F, Matute G, et al. (2003) Iron, zinc and iodide status in Mexican children under 12 years and women 12–49 years of age. A probabilistic national survey. Salud Publica Mex 45 Suppl 4S520–529. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
