

Reproducibility of scleral spur identification and angle measurements using fourier domain anterior segment optical coherence tomography
- PMID: 23209880
- PMCID: PMC3503366
- DOI: 10.1155/2012/487309
Reproducibility of scleral spur identification and angle measurements using fourier domain anterior segment optical coherence tomography
Abstract
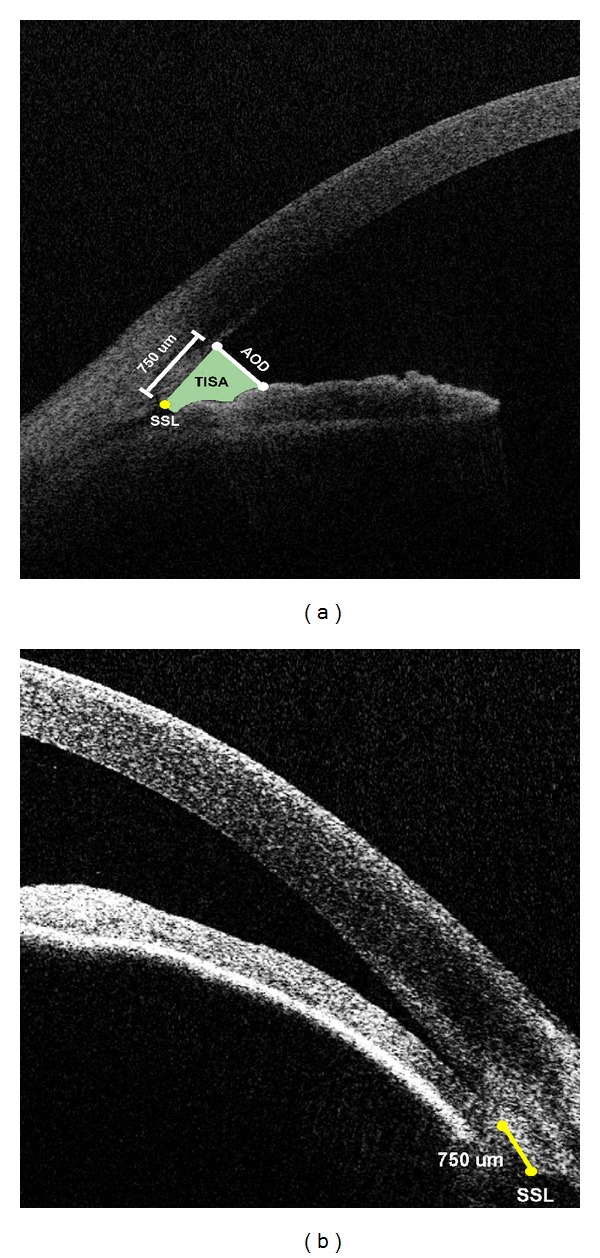
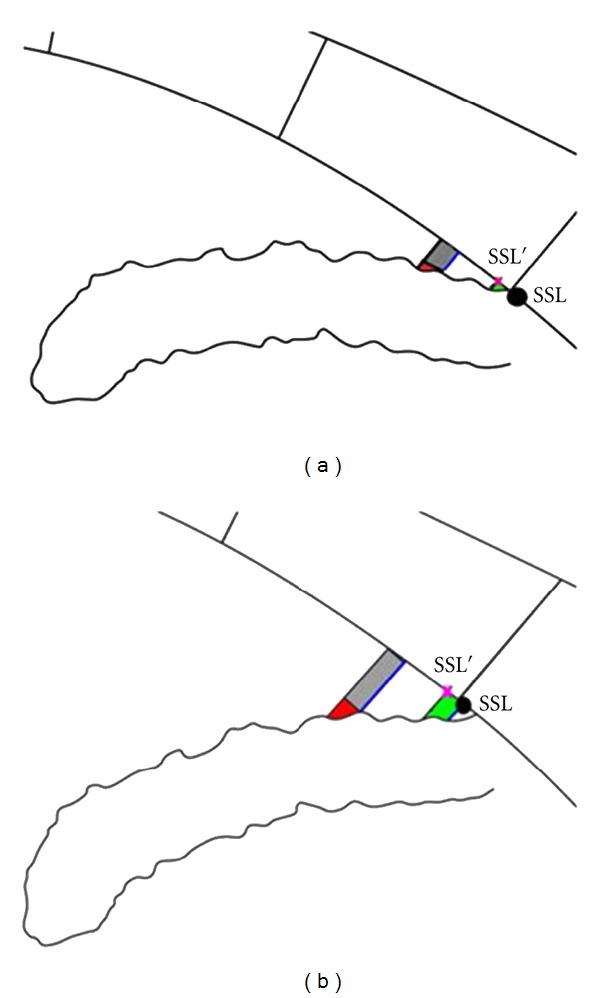
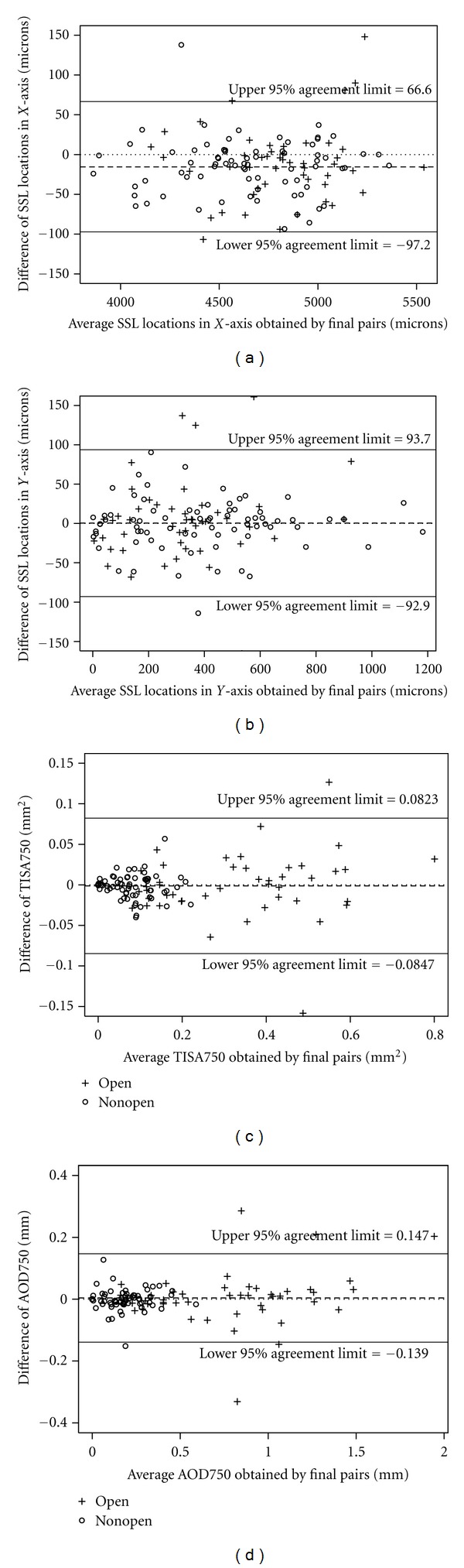
Purpose. To evaluate intraobserver and interobserver agreement in locating the scleral spur landmark (SSL) and anterior chamber angle measurements obtained using Fourier Domain Anterior Segment Optical Coherence Tomography (ASOCT) images. Methods. Two independent, masked observers (SR and AZC) identified SSLs on ASOCT images from 31 eyes with open and nonopen angles. A third independent reader, NPB, adjudicated SSL placement if identifications differed by more than 80 μm. Nine months later, SR reidentified SSLs. Intraobserver and interobserver agreement in SSL placement, trabecular-iris space area (TISA750), and angle opening distance (AOD750) were calculated. Results. In 84% of quadrants, SR's SSL placements during 2 sessions were within 80 μm in both the X- and Y-axes, and in 77% of quadrants, SR and AZC were within 80 μm in both axes. In adjudicated images, 90% of all quadrants were within 80 μm, 88% in nonopen-angle eyes, and 92% in open-angle eyes. The intraobserver and interobserver correlation coefficients (with and without adjudication) were above 0.9 for TISA750 and AOD750 for all quadrants. Conclusions. Reproducible identification of the SSL from images obtained with FD-ASOCT is possible. The ability to identify the SSL allows reproducible measurement of the anterior chamber angle using TISA750 and AOD750.
Figures
References
-
- Nolan W. Anterior segment imaging: ultrasound biomicroscopy and anterior segment optical coherence tomography. Current Opinion in Ophthalmology. 2008;19(2):115–121. - PubMed
-
- Friedman DS, He M. Anterior chamber angle assessment techniques. Survey of Ophthalmology. 2008;53(3):250–273. - PubMed
-
- American Academy of Ophthalmology. Primary Angle Closure, Preferred Practice Pattern. San Francisco, Calif, USA: American Academy of Ophthalmology; 2010.
-
- Izatt JA, Hee MR, Swanson EA, et al. Micrometer-scale resolution imaging of the anterior eye in vivo with optical coherence tomography. Archives of Ophthalmology. 1994;112(12):1584–1589. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
