

Reviewing long-term antidepressants can reduce drug burden: a prospective observational cohort study
- PMID: 23211181
- PMCID: PMC3481518
- DOI: 10.3399/bjgp12X658304
Reviewing long-term antidepressants can reduce drug burden: a prospective observational cohort study
Abstract
Background: Antidepressant prescribing continues to rise. Contributing factors are increased long-term prescribing and possibly the use of higher selective serotonin re-uptake inhibitor (SSRI) doses.
Aim: To review general practice patients prescribed the same antidepressant long-term (≥2 years) and evaluate prescribing and management pre and post-review.
Design and setting: Prospective observational cohort study using routine data from 78 urban general practices, Scotland.
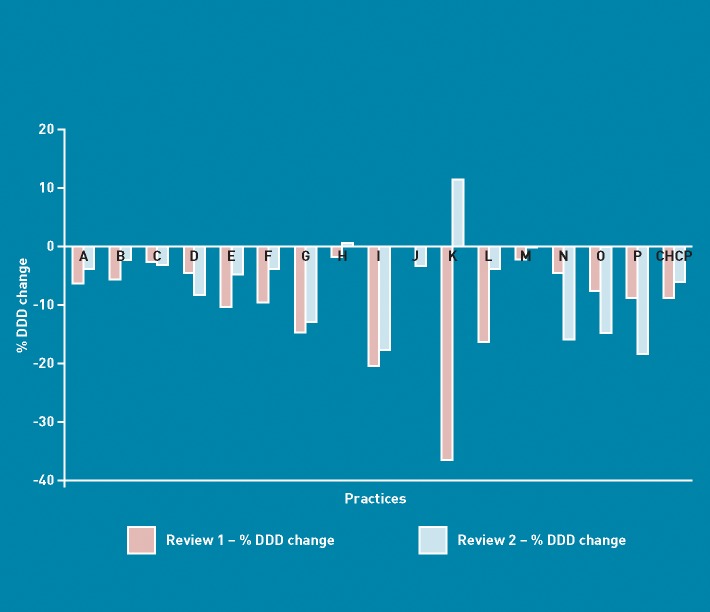
Method: All patients prescribed antidepressants (excluding amitriptyline) for ≥2 years were identified from records November 2009 to March 2010. GPs selected patients for face-to-face review of clinical condition and medication, December 2009 to September 2010. Pre- and post-review data were collected; average antidepressant doses and changes in prescribed daily doses were calculated. Onward referral to support services was recorded.
Results: 8.6% (33 312/388 656) of all registered patients were prescribed an antidepressant, 47.1% (15 689) were defined as long-term users and 2849 (18.2%) were reviewed. 811 (28.5%) patients reviewed had a change in antidepressant therapy: 7.0% stopped, 12.8% reduced dose, 5.3% increased dose, and 3.4% changed antidepressant, resulting in 9.5% (95% CI = 9.1% to 9.8% P<0.001) reduction in prescribed daily dose and 8.1% reduction in prescribing costs. 6.3% were referred onwards, half to NHS Mental Health Services. Pre-review SSRI doses were 10-30% higher than previously reported.
Conclusion: Almost half of all people prescribed antidepressants were long-term users. Appropriate reductions in prescribing can be achieved by reviewing patients. Higher SSRI doses may be contributing to current antidepressant growth.
Figures
References
-
- Middleton N, Gunnell D, Whitley E, et al. Secular trends in antidepressant prescribing in the UK, 1975–1998. J Public Health Med. 2001;23(4):262–267. - PubMed
-
- Mental health policy and practice across Europe: the future direction of mental health care. Maidenhead: McGraw-Hill, Open University Press; 2007.
-
- Chen Y, Kelton CM, Jing Y, et al. Utilization, price, and spending trends for antidepressants in the US Medicaid Program. Res Social Adm Pharm. 2008;4(3):244–257. - PubMed
-
- Poluzzi E, Motola D, Silvani C, et al. Prescriptions of antidepressants in primary care in Italy: pattern of use after admission of selective serotonin reuptake inhibitors for reimbursement. Eur J Clin Pharmacol. 2004;59(11):825–831. - PubMed
-
- Information Services Division, Scotland. Antidepressants. Edinburgh: ISD Scotland; 2011. http://www.isdscotlandarchive.scot.nhs.uk/isd/information-and-statistics... (accessed 19 Sep 2012)