

Wireless insufflation of the gastrointestinal tract
- PMID: 23212312
- PMCID: PMC3850772
- DOI: 10.1109/TBME.2012.2230631
Wireless insufflation of the gastrointestinal tract
Abstract
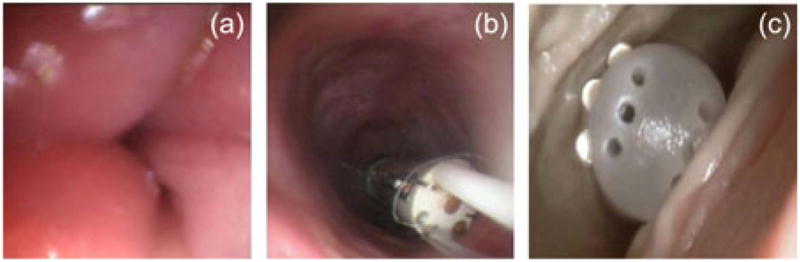
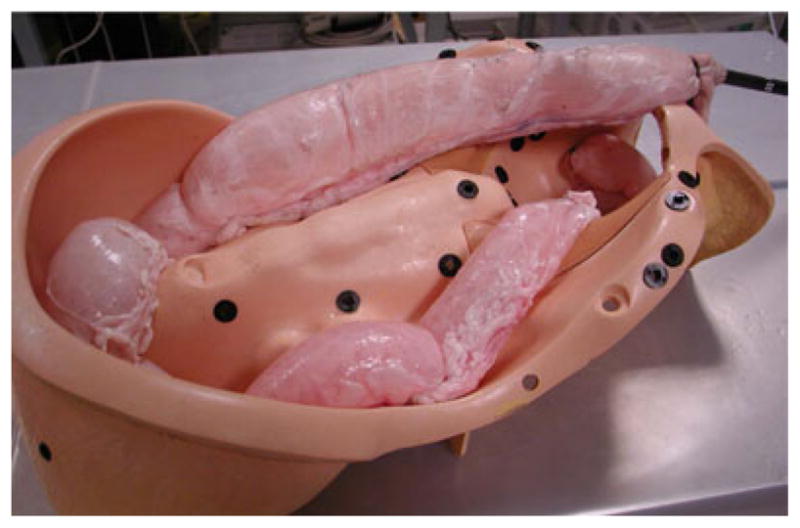
Despite clear patient experience advantages, low specificity rates have thus far prevented swallowable capsule endoscopes from replacing traditional endoscopy for diagnosis of colon disease. One explanation for this is that capsule endoscopes lack the ability to provide insufflation, which traditional endoscopes use to distend the intestine for a clear view of the internal wall. To provide a means of insufflation from a wireless capsule platform, in this paper we use biocompatible effervescent chemical reactions to convert liquids and powders carried onboard a capsule into gas. We experimentally evaluate the quantity of gas needed to enhance capsule visualization and locomotion, and determine how much gas can be generated from a given volume of reactants. These experiments motivate the design of a wireless insufflation capsule, which is evaluated in ex vivo experiments. These experiments illustrate the feasibility of enhancing visualization and locomotion of endoscopic capsules through wireless insufflation.
Figures











References
-
- Toennies JL, Ciuti G, Smith BF, Menciassi A, Valdastri P, Webster RJ., III Toward tetherless insufflation of the GI tract. Proc Int Conf IEEE Eng Med Biol Soc. 2010 Aug-Sep;:1946–1949. - PubMed
-
- Toennies JL, Webster RJ., III A wireless insufflation system for capsular endoscopes. J Med Dev. 2009 Jun;3(2):27514.
-
- American Cancer Society. What are the key statistics about colorectal cancer? 2012 Aug; [Online]. Available: http://www.cancer.org/Cancer/ColonandRectumCancer/DetailedGuide/colorect....
-
- Joseph DA, DeGroff AS, Hayes NS, Wong FL, Plescia M. The colorectal cancer control program: Partnering to increase population level screening. Gastroint Endosc. 2011;73(3):429–434. - PubMed
-
- Winawer SJ. Colorectal cancer screening. Best Pract Res Clin Gastroenterol. 2007;21:1031–1048. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
