

Lateralized reverse shoulder arthroplasty maintains rotational function of the remaining rotator cuff
- PMID: 23212769
- PMCID: PMC3563780
- DOI: 10.1007/s11999-012-2692-x
Lateralized reverse shoulder arthroplasty maintains rotational function of the remaining rotator cuff
Abstract
Background: Humeral rotation often remains compromised after nonlateralized reverse shoulder arthroplasty (RSA). Reduced rotational moment arms and muscle slackening have been identified as possible reasons for this impairment. Although several clinical studies suggest lateralized RSA may increase rotation, it is unclear whether this is attributable to preservation of rotational moment arms and muscle pretension of the remaining rotator cuff.
Questions/purposes: The lateralized RSA was analyzed to determine whether (1) the rotational moment arms and (2) the origin-to-insertion distances of the teres minor and subscapularis can be preserved, and (3) their flexion and abduction moment arms are decreased.
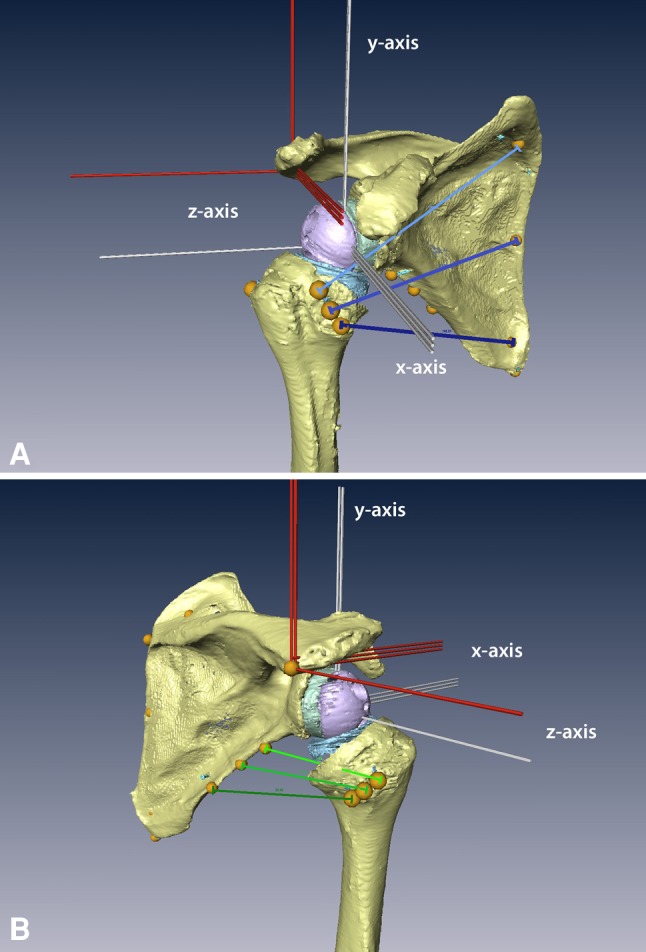
Methods: Lateralized RSA using an 8-mm resin block under the glenosphere was performed on seven cadaveric shoulder specimens. Preimplantation and postimplantation CT scans were obtained to create three-dimensional shoulder surface models. Using these models, function-specific moment arms and origin-to-insertion distances of three segments of the subscapularis and teres minor muscles were calculated.
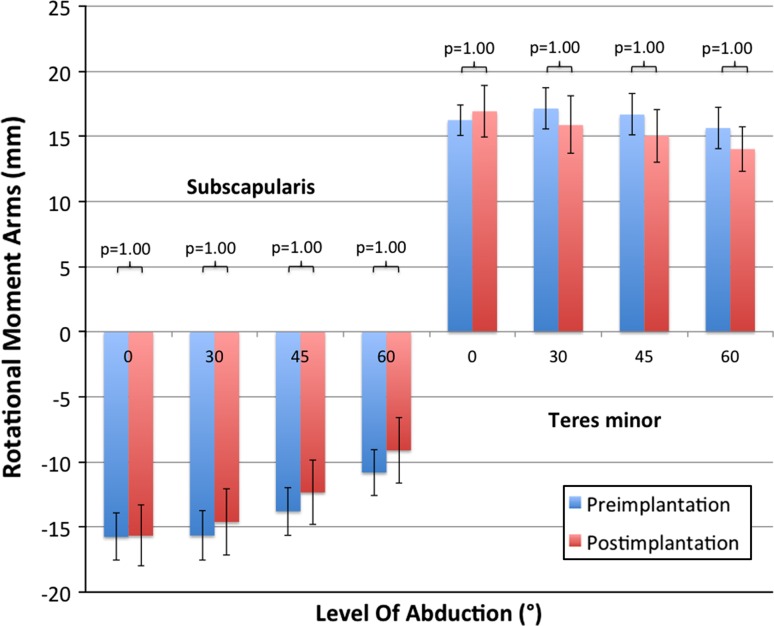
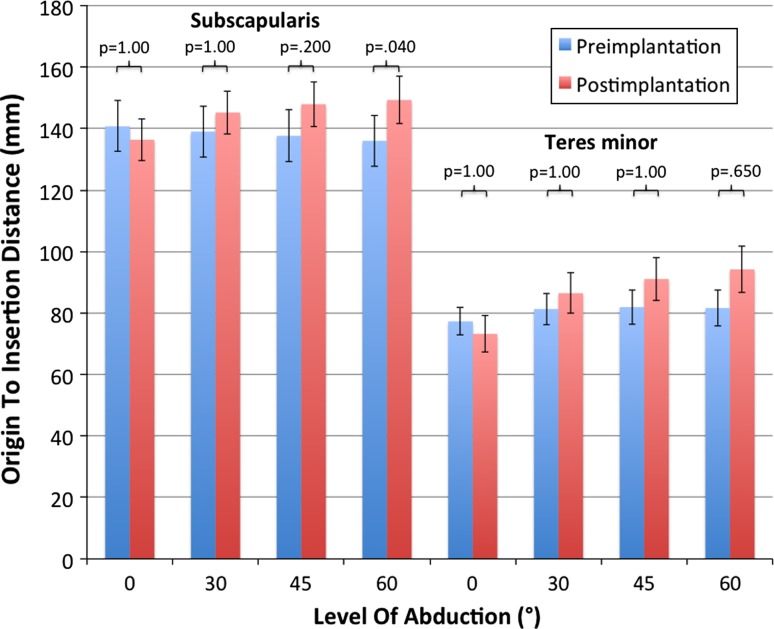
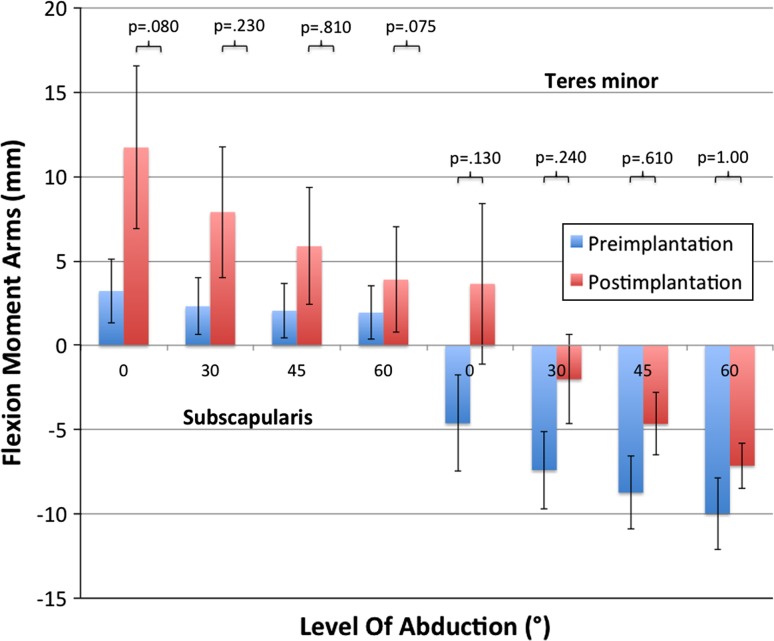
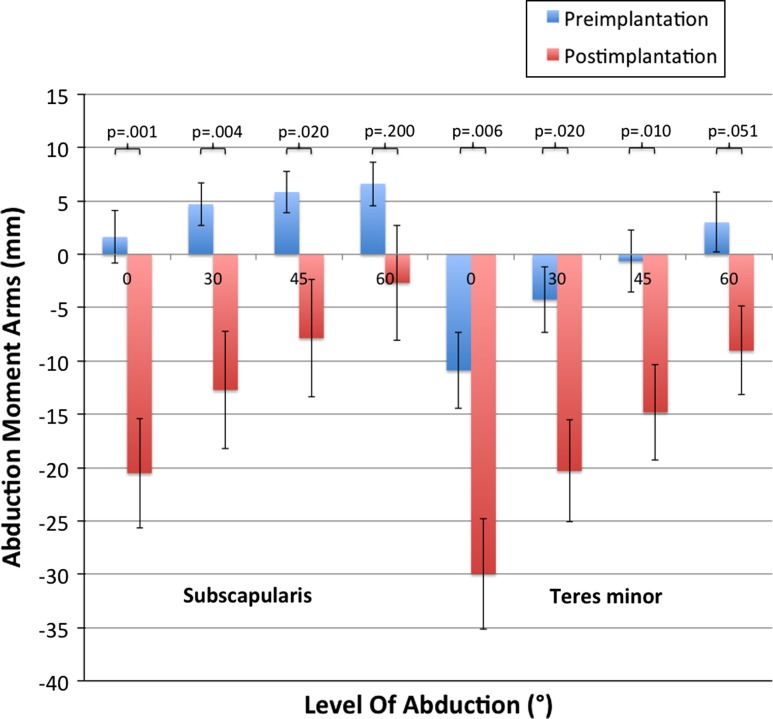
Results: The rotational moment arms remained unchanged for the middle and caudal subscapularis and teres minor segments in all tested positions (subscapularis, -16.1 mm versus -15.8 mm; teres minor, 15.9 mm versus 15.3 mm). The origin-to-insertion distances increased or remained unchanged in any muscle segment apart from the distal subscapularis segment at 0° abduction (139 mm versus 145 mm). The subscapularis and teres minor had increased flexion moment arms in abduction angles smaller than 60° (subscapularis, 2.7 mm versus 8.3 mm; teres minor, -6.6 mm versus 0.8 mm). Abduction moment arms decreased for all segments (subscapularis, 4 mm versus -11 mm; teres minor, -3.6 mm versus -19 mm).
Conclusions: After lateralized RSA, the subscapularis and teres minor maintained their length and rotational moment arms, their flexion forces were increased, and abduction capability decreased.
Clinical relevance: Our findings could explain clinically improved rotation in lateralized RSA in comparison to nonlateralized RSA.
Figures
References
-
- Boileau P, Chuinard C, Roussanne Y, Bicknell RT, Rochet N, Trojani C. Reverse shoulder arthroplasty combined with a modified latissimus dorsi and teres major tendon transfer for shoulder pseudoparalysis associated with dropping arm. Clin Orthop Relat Res. 2008;466:584–593. doi: 10.1007/s11999-008-0114-x. - DOI - PMC - PubMed
-
- Boileau P, Chuinard C, Roussanne Y, Neyton L, Trojani C. Modified latissimus dorsi and teres major transfer through a single delto-pectoral approach for external rotation deficit of the shoulder: as an isolated procedure or with a reverse arthroplasty. J Shoulder Elbow Surg. 2007;16:671–682. doi: 10.1016/j.jse.2007.02.127. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
