

doi: 10.3747/pdi.2012.00152.
Posterior reversible encephalopathy syndrome: a truly treatable neurologic illness
Affiliations
- PMID: 23212858
- PMCID: PMC3524908
- DOI: 10.3747/pdi.2012.00152
Item in Clipboard
Posterior reversible encephalopathy syndrome: a truly treatable neurologic illness
Perit Dial Int.
2012 Nov-Dec.
No abstract available
Figures
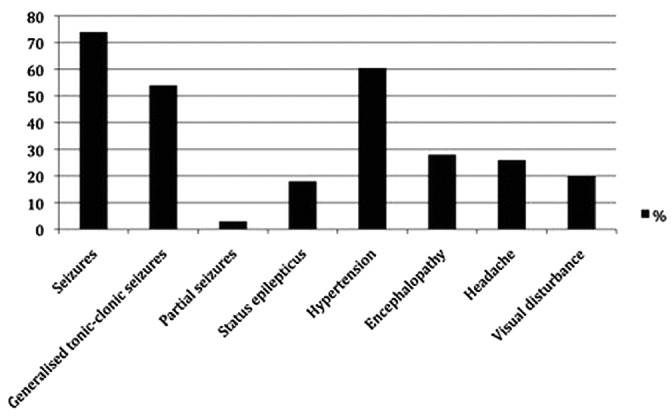
— Frequency of posterior reversible encephalopathy syndrome signs and symptoms seen in a series of 120 cases (4).
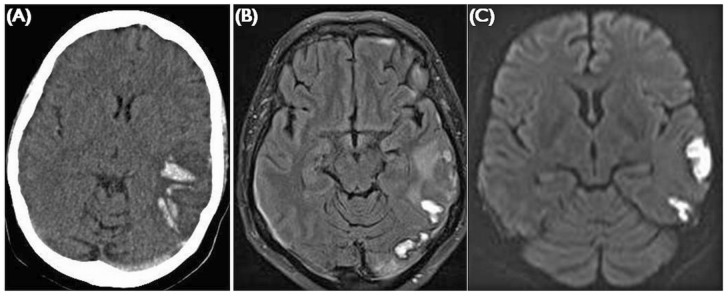
— Venous sinus thrombosis. (A) Unenhanced computed tomography shows posterior temporal parenchymal hemorrhage and a hyperdense left transverse sinus. (B) FLAIR (fluid attenuated inversion recovery) imaging shows high signal in the area of hemorrhage, with vasogenic edema in the white matter. (C) Diffusion-weighted imaging can be confounded in areas of hemorrhage, giving a picture of apparent restriction. Findings are usually unilateral and restricted to a venous drainage territory.
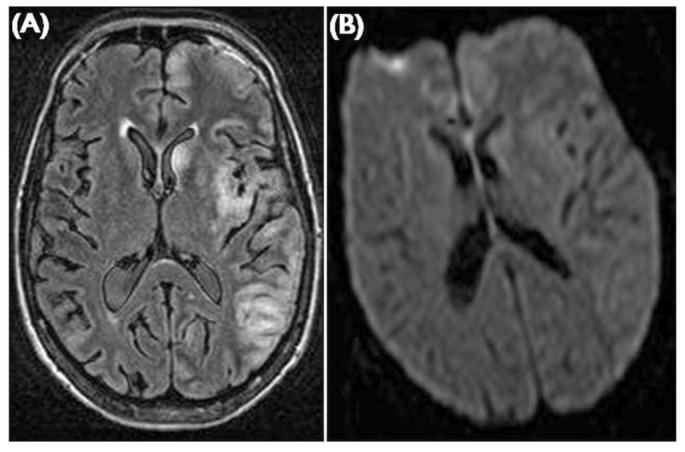
— Herpes simplex encephalitis. (A) In this case, FLAIR (fluid attenuated inversion recovery) imaging shows high signal in the left insular cortex, posterior temporal lobe, cingulate gyrus, and caudate nucleus. Findings are usually bilateral and asymmetrical, and can mimic an atypical posterior reversible encephalopathy syndrome with frontal distribution. (B) Diffusion weighted changes can also occur.
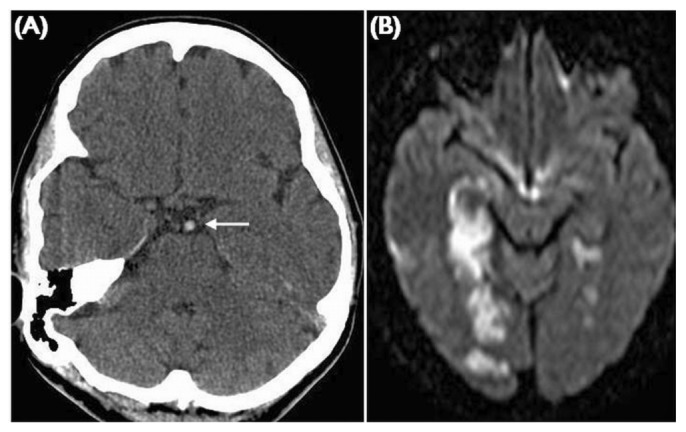
— Basilar artery thrombosis. (A) Unenhanced computed tomography demonstrates a hyperdense basilar artery indicating acute thrombus (white arrow). The diffusion weighted imaging shows bilateral posterior circulation infarcts involving the white and grey matter.
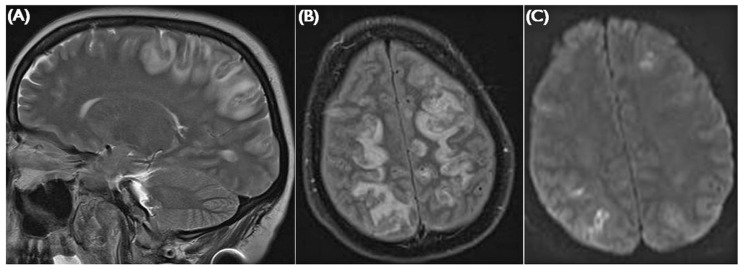
— Posterior reversible encephalopathy syndrome. (A) Sagittal T2-weighted image shows the distribution of subcortical edema typically involving the posterior frontal, parietal, and occipital lobes. (B) Axial FLAIR (fluid attenuated inversion recovery) imaging eloquently demonstrates the subcortical edema. (C) B1000 images from a diffusion-weighted sequence shows restricted diffusion in the cortex. Findings are usually bilateral and asymmetrical.
References
-
- McKinney AM, Short J, Truwit CL, McKinney ZJ, Kozak OS, SantaCruz KS, et al. Posterior reversible encephalopathy syndrome: incidence of atypical regions of involvement and imaging findings. AJR Am J Roentgenol 2007; 189:904–12 - PubMed
-
- Roth C, Ferbert A. The posterior reversible encephalopathy syndrome: what’s certain, what’s new? Pract Neurol 2011; 11:136–44 - PubMed
-
- Hinchey J, Chaves C, Appignani B, Breen J, Pao L, Wang A, et al. A reversible posterior leukoencephalopathy syndrome. N Engl J Med 1996; 334:494–500 - PubMed
-
- Gokce M, Dogan E, Nacitarhan S, Demirpolat G. Posterior reversible encephalopathy syndrome caused by hypertensive encephalopathy and acute uremia. Neurocrit Care 2006; 4:133–6 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
