

Biomechanics of lateral interbody spacers: going wider for going stiffer
- PMID: 23213284
- PMCID: PMC3504399
- DOI: 10.1100/2012/381814
Biomechanics of lateral interbody spacers: going wider for going stiffer
Abstract
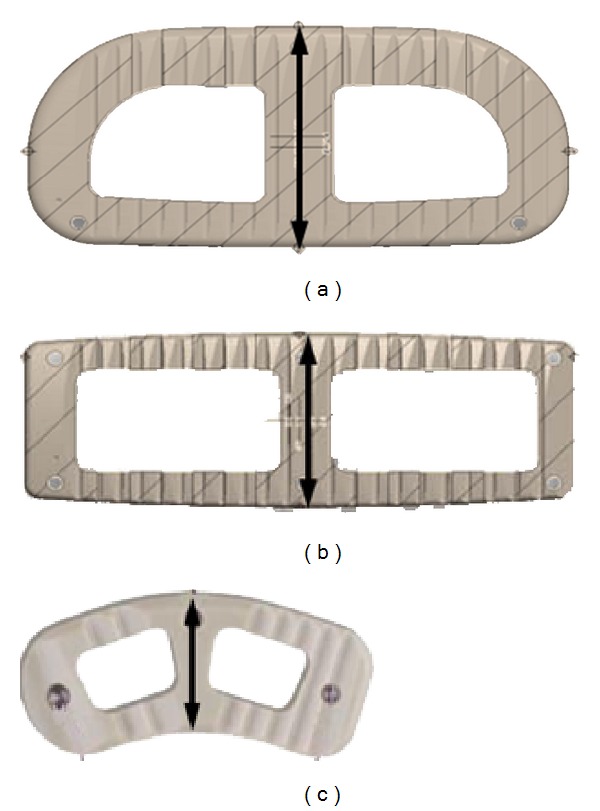
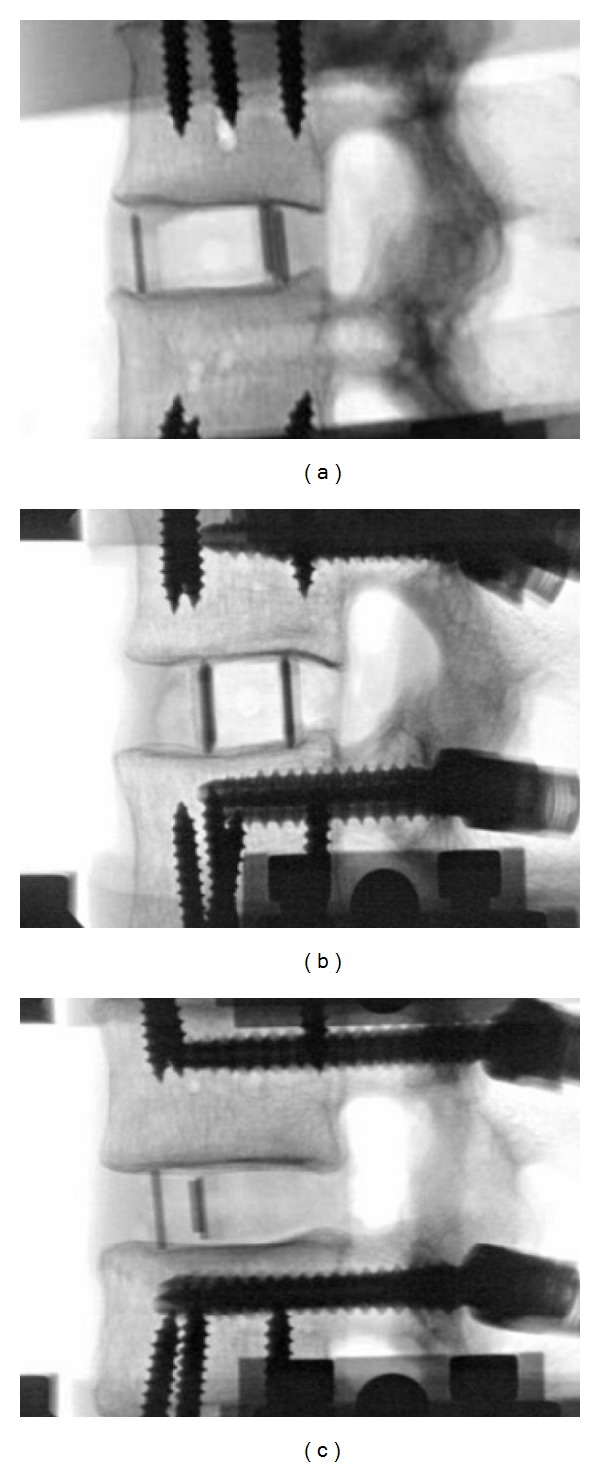
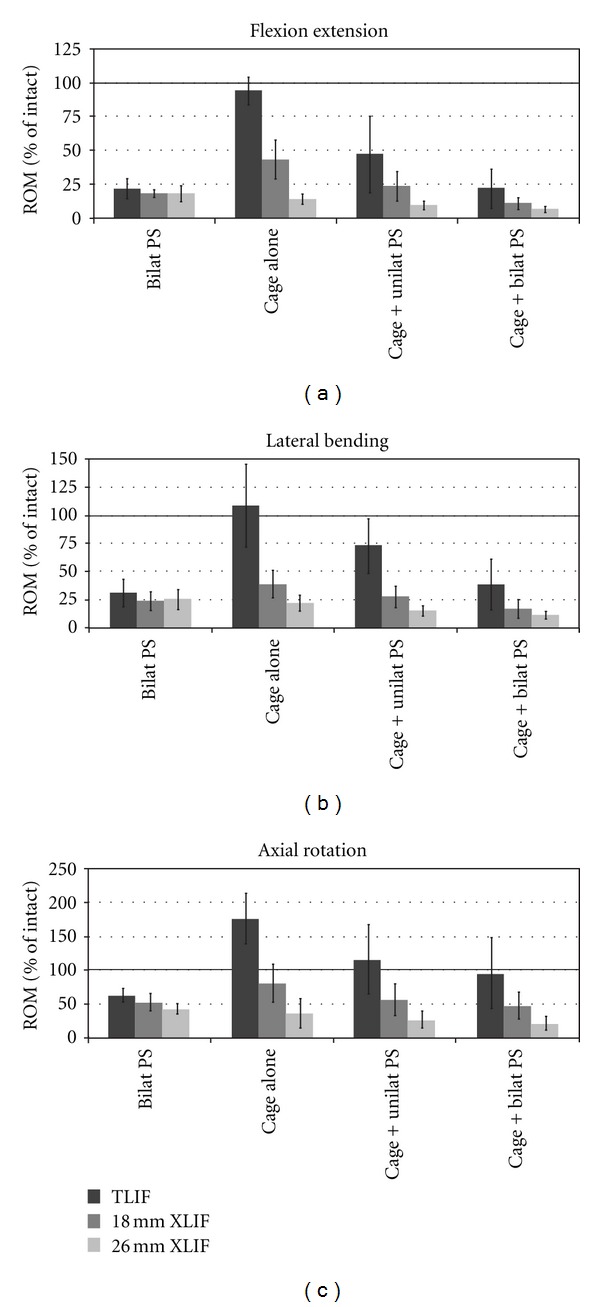
This study investigates the biomechanical stability of a large interbody spacer inserted by a lateral approach and compares the biomechanical differences with the more conventional transforaminal interbody fusion (TLIF), with and without supplemental pedicle screw (PS) fixation. Twenty-four L2-L3 functional spinal units (FSUs) were tested with three interbody cage options: (i) 18 mm XLIF cage, (ii) 26 mm XLIF cage, and (iii) 11 mm TLIF cage. Each spacer was tested without supplemental fixation, and with unilateral and bilateral PS fixation. Specimens were subjected to multidirectional nondestructive flexibility tests to 7.5 N·m. The range of motion (ROM) differences were first examined within the same group (per cage) using repeated-measures ANOVA, and then compared between cage groups. The 26 mm XLIF cage provided greater stability than the 18 mm XLIF cage with unilateral PS and 11 mm TLIF cage with bilateral PS. The 18 mm XLIF cage with unilateral PS provided greater stability than the 11 mm TLIF cage with bilateral PS. This study suggests that wider lateral spacers are biomechanically stable and offer the option to be used with less or even no supplemental fixation for interbody lumbar fusion.
Figures
References
-
- Elowitz EH, Yanni DS, Chwajol M, Starke RM, Perin NI. Evaluation of indirect decompression of the lumbar spinal canal following minimally invasive lateral transpsoas interbody fusion: radiographic and outcome analysis. Minimally Invasive Neurosurgery. 2011;54(5-6):201–206. - PubMed
-
- Isaacs RE, Hyde J, Goodrich JA, Rodgers WB, Phillips FM. A prospective, nonrandomized, multicenter evaluation of extreme lateral interbody fusion for the treatment of adult degenerative scoliosis: perioperative outcomes and complications. Spine. 2010;35(supplement 26):S322–S330. - PubMed
-
- Oliveira L, Marchi L, Coutinho E, Pimenta L. A radiographic assessment of the ability of the extreme lateral interbody fusion procedure to indirectly decompress the neural elements. Spine. 2010;35(supplement 26):S331–S337. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
