

Navigating the difficult robotic assisted pyeloplasty
- PMID: 23213571
- PMCID: PMC3503323
- DOI: 10.5402/2012/291235
Navigating the difficult robotic assisted pyeloplasty
Abstract
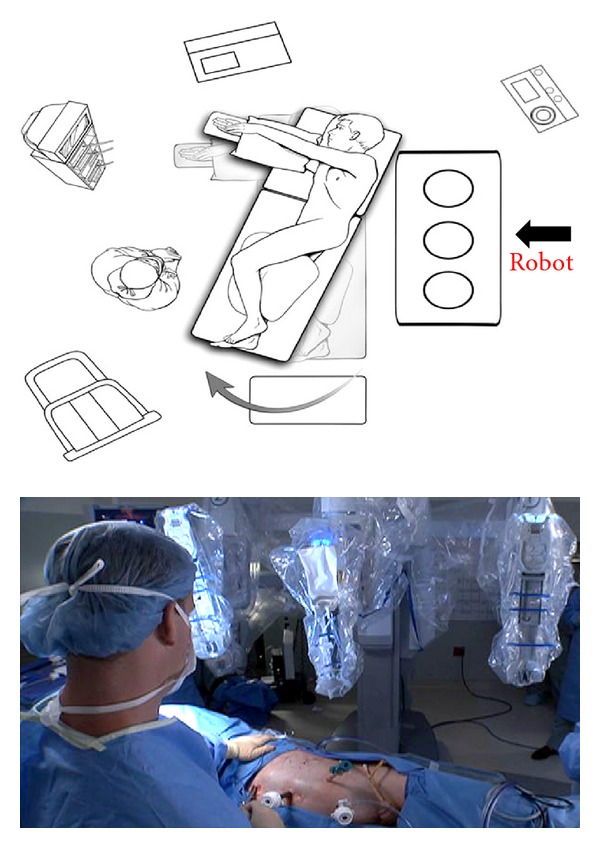
Pyeloplasty is the gold standard therapy for ureteropelvic junction obstruction. Robotic assisted pyeloplasty has been widely adopted by urologists with and without prior laparoscopic pyeloplasty experience. However, difficult situations encountered during robotic assisted pyeloplasty can significantly add to the difficulty of the operation. This paper provides tips for patient positioning, port placement, robot docking, and intraoperative dissection and repair in patients with the difficult situations of obesity, large floppy liver, difficult to reflect colon (transmesenteric pyeloplasty), crossing vessels, large calculi, and previous attempts at ureteropelvic junction repair. Techniques presented in this paper may aid in the successful completion of robotic assisted pyeloplasty in the face of the difficult situations noted above.
Figures

References
-
- Mufarrij PW, Woods M, Shah OD, et al. Robotic dismembered pyeloplasty: a 6-year, multi-institutional experience. Journal of Urology. 2008;180(4):1391–1396. - PubMed
-
- Gupta NP, Nayyar R, Hemal AK, Mukherjee S, Kumar R, Dogra PN. Outcome analysis of robotic pyeloplasty: a large single-centre experience. BJU International. 2010;105(7):980–983. - PubMed
-
- Singh I, Hemal AK. Robot-assisted pyeloplasty: review of the current literature, technique and outcome. The Canadian journal of urology. 2010;17(2):5099–5108. - PubMed
-
- Thiel DD, Winfield HN. Robotic assisted laparoscopic pyeloplasty. Minerva Urologica e Nefrologica. 2007;59(2):167–177. - PubMed
-
- Thiel DD, Leroy JL, Winfield HN, Igel TC. Roboticassisted laparoscopic reconstruction of the upper urinary tract: tips and tricks. Urology. 2010;76(2):488–493. - PubMed
LinkOut - more resources
Full Text Sources