

Complications in the treatment of intracranial aneurysms with silk stents: an analysis of 30 consecutive patients
- PMID: 23217636
- PMCID: PMC3520555
- DOI: 10.1177/159101991201800407
Complications in the treatment of intracranial aneurysms with silk stents: an analysis of 30 consecutive patients
Abstract
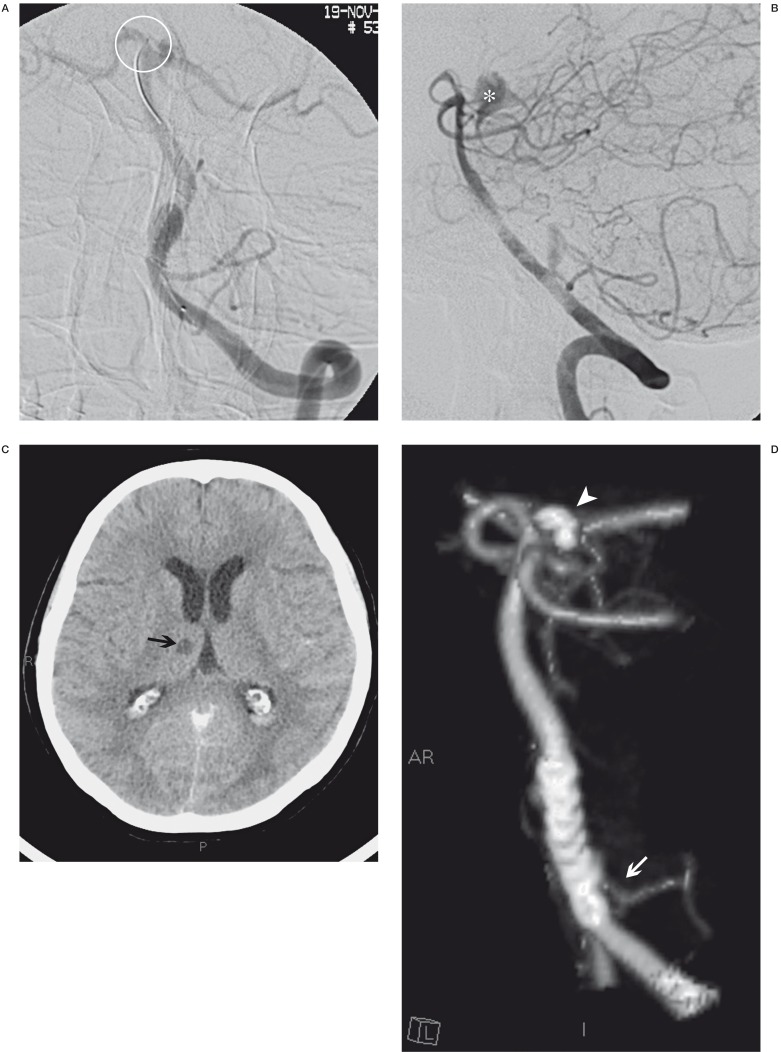
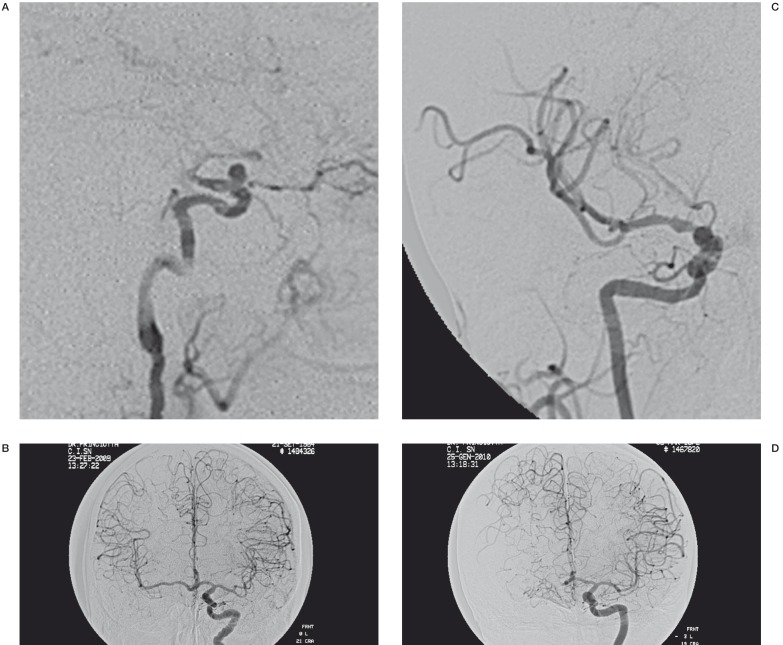
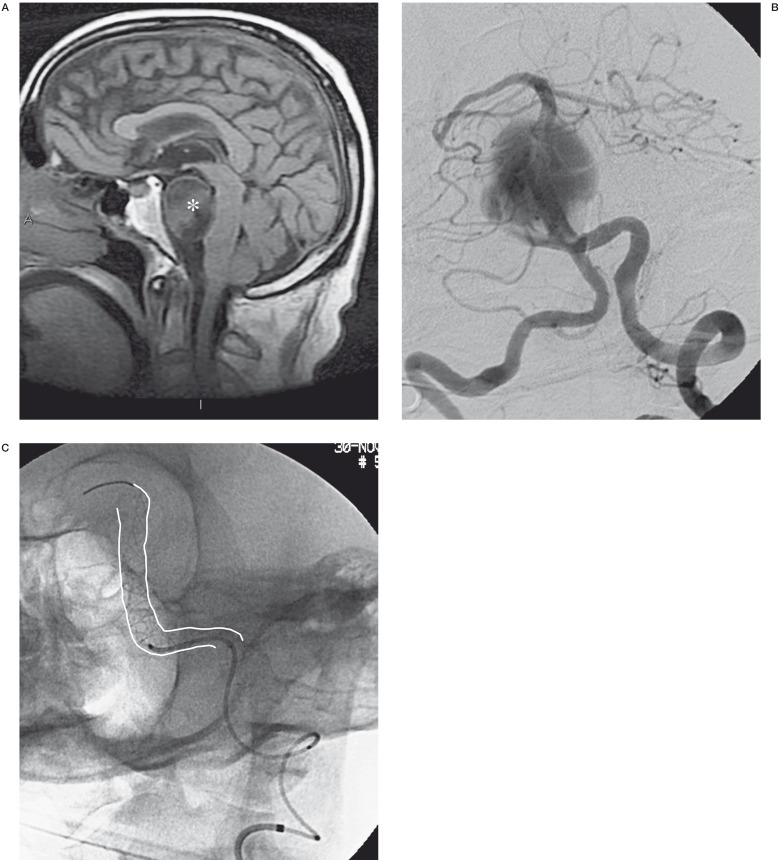
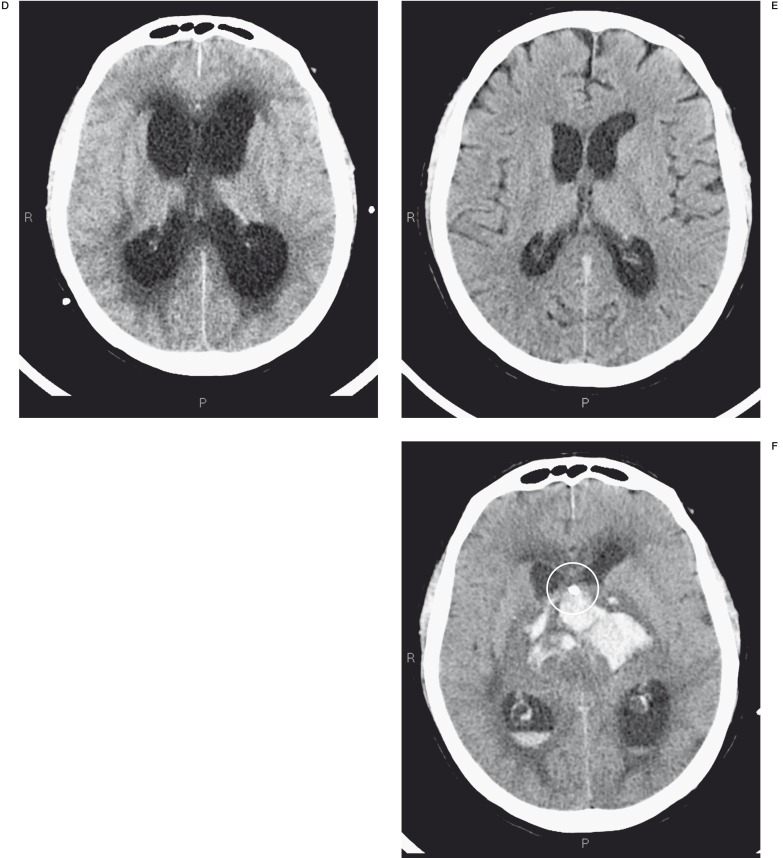
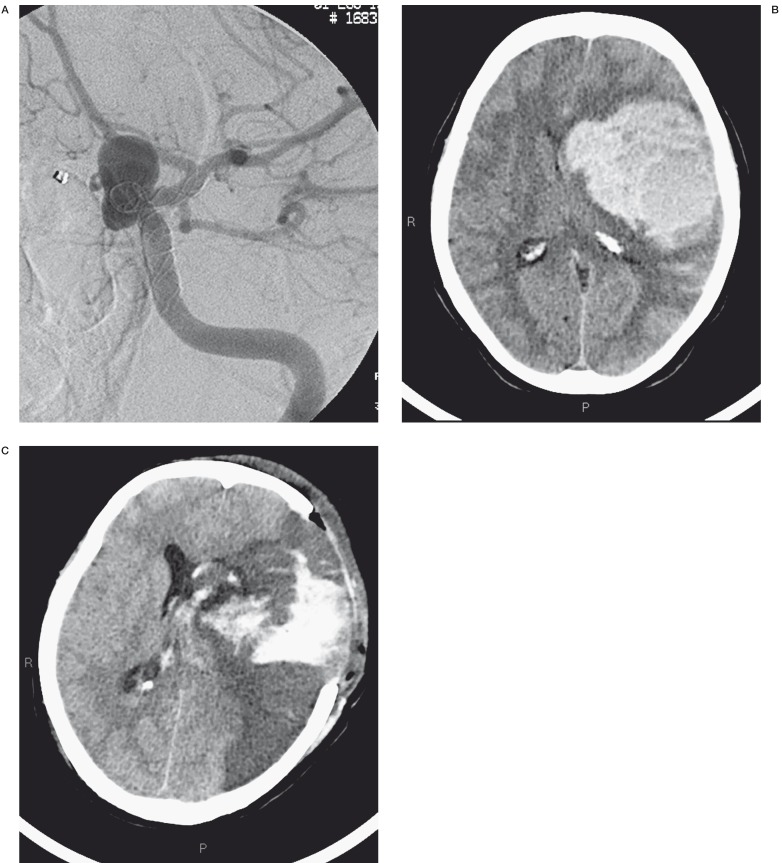
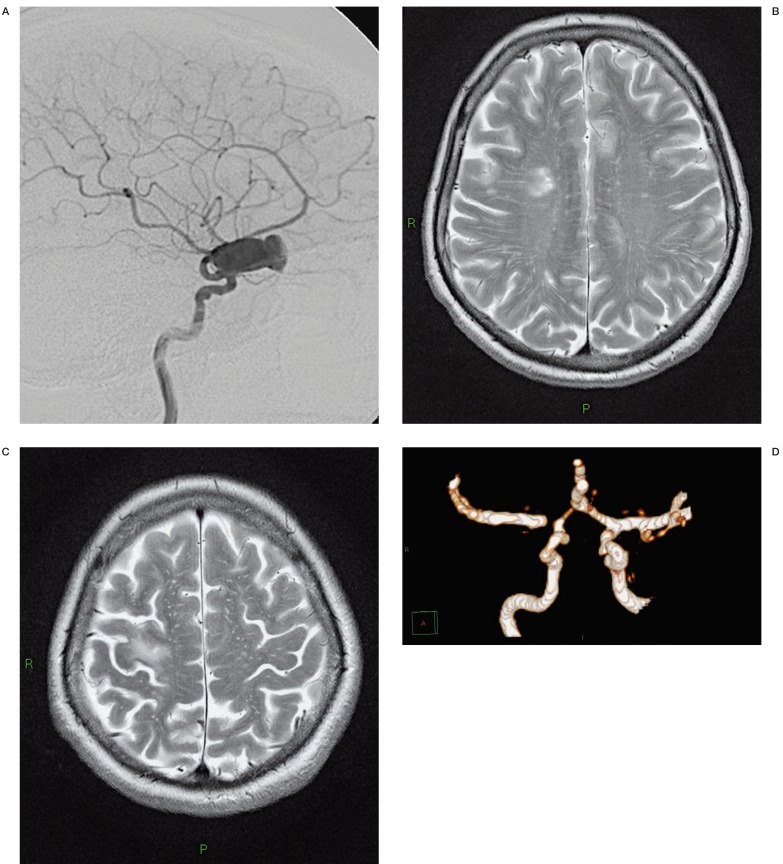
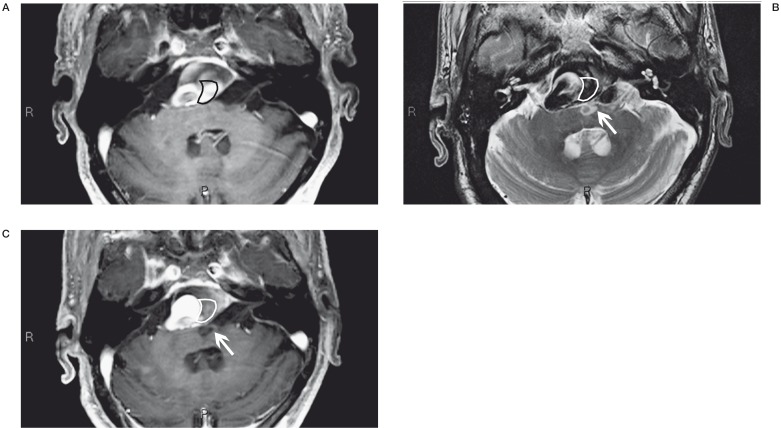
Flow-diverting stents (Silk and PED) have radically changed the approach to intracranial aneurysm treatment from the use of endosaccular materials to use of an extraaneurysmal endoluminal device. However, much debate surrounds the most appropriate indications for the use of FD stents and the problems raised by several possible complications.We analysed our technical difficulties and the early (less than ten days after treatment) and late complications encountered in 30 aneurysms treated comprising 13 giant lesions, 12 large, five with maximum diameters <10 mm and one blister-like aneurysm. In our experience the primary indications for the use of FD stents can be the symptomatic intracavernous giant aneurysms. Although the extracavernous carotid siphon aneurysms have major risk of bleeding, FD stents are indicated clearly explaining the risks to the patient in case of severe mass effect. There is a very complex assessment for aneurysms of the vertebrobasilar circulation.
Figures


Similar articles
-
Treatment of complex intracranial aneurysms using flow-diverting silk® stents. An analysis of 32 consecutive patients.Interv Neuroradiol. 2014 Dec;20(6):729-35. doi: 10.15274/INR-2014-10070. Epub 2014 Dec 5. Interv Neuroradiol. 2014. PMID: 25496683 Free PMC article.
-
Treatment of intracranial aneurysms using flow-diverting silk stents (BALT): a single centre experience.Interv Neuroradiol. 2011 Sep;17(3):306-15. doi: 10.1177/159101991101700305. Epub 2011 Oct 17. Interv Neuroradiol. 2011. PMID: 22005692 Free PMC article. Clinical Trial.
-
Panacea or problem: flow diverters in the treatment of symptomatic large or giant fusiform vertebrobasilar aneurysms.J Neurosurg. 2012 Jun;116(6):1258-66. doi: 10.3171/2012.2.JNS111942. Epub 2012 Mar 9. J Neurosurg. 2012. PMID: 22404673
-
The Silk flow-diverter stent for endovascular treatment of intracranial aneurysms.Expert Rev Med Devices. 2015;12(6):753-62. doi: 10.1586/17434440.2015.1093413. Epub 2015 Sep 28. Expert Rev Med Devices. 2015. PMID: 26415045 Review.
-
Endovascular treatment of complex intracranial aneurysms by pipeline flow-diverter embolization device: a single-center experience.Neurol Res. 2015 Apr;37(4):359-65. doi: 10.1179/1743132814Y.0000000450. Epub 2014 Oct 13. Neurol Res. 2015. PMID: 25310354 Review.
Cited by
-
Should we still consider clips for basilar apex aneurysms? A critical appraisal of the literature.Surg Neurol Int. 2018 Feb 21;9:44. doi: 10.4103/sni.sni_311_17. eCollection 2018. Surg Neurol Int. 2018. PMID: 29541485 Free PMC article. Review.
-
Silk® Flow Diverter Device for Intracranial Aneurysm Treatment: A Systematic Review and Meta-Analysis.Neurointervention. 2021 Nov;16(3):222-231. doi: 10.5469/neuroint.2021.00234. Epub 2021 Sep 14. Neurointervention. 2021. PMID: 34517469 Free PMC article. Review.
-
Delayed hemorrhagic complications after flow diversion for intracranial aneurysms: a literature overview.Neuroradiology. 2016 Feb;58(2):171-7. doi: 10.1007/s00234-015-1615-4. Epub 2015 Nov 9. Neuroradiology. 2016. PMID: 26553302 Free PMC article.
-
Treatment of vertebrobasilar fusiform aneurysms with Pipeline embolization device.Interv Neuroradiol. 2015 Aug;21(4):434-40. doi: 10.1177/1591019915590068. Epub 2015 Jun 18. Interv Neuroradiol. 2015. PMID: 26089246 Free PMC article.
-
Preclinical Testing of a Novel Thin Film Nitinol Flow-Diversion Stent in a Rabbit Elastase Aneurysm Model.AJNR Am J Neuroradiol. 2016 Mar;37(3):497-501. doi: 10.3174/ajnr.A4568. Epub 2015 Oct 22. AJNR Am J Neuroradiol. 2016. PMID: 26494695 Free PMC article.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
