

Comparison of longer-term safety and effectiveness of 4 atypical antipsychotics in patients over age 40: a trial using equipoise-stratified randomization
- PMID: 23218100
- PMCID: PMC3600635
- DOI: 10.4088/JCP.12m08001
Comparison of longer-term safety and effectiveness of 4 atypical antipsychotics in patients over age 40: a trial using equipoise-stratified randomization
Abstract
Objective: To compare longer-term safety and effectiveness of the 4 most commonly used atypical antipsychotics (aripiprazole, olanzapine, quetiapine, and risperidone) in 332 patients, aged > 40 years, having psychosis associated with schizophrenia, mood disorders, posttraumatic stress disorder, or dementia, diagnosed using DSM-IV-TR criteria.
Method: We used equipoise-stratified randomization (a hybrid of complete randomization and clinician's choice methods) that allowed patients or their treating psychiatrists to exclude 1 or 2 of the study atypical antipsychotics due to past experience or anticipated risk. Patients were followed for up to 2 years, with assessments at baseline, 6 weeks, 12 weeks, and every 12 weeks thereafter. Medications were administered employing open-label design and flexible dosages, but with blind raters. The study was conducted from October 2005 to October 2010.
Outcome measures: Primary metabolic markers (body mass index, blood pressure, fasting blood glucose, low-density lipoprotein cholesterol, high-density lipoprotein cholesterol, and triglycerides), percentage of patients who stay on the randomly assigned atypical antipsychotic for at least 6 months, psychopathology, percentage of patients who develop metabolic syndrome, and percentage of patients who develop serious and nonserious adverse events.
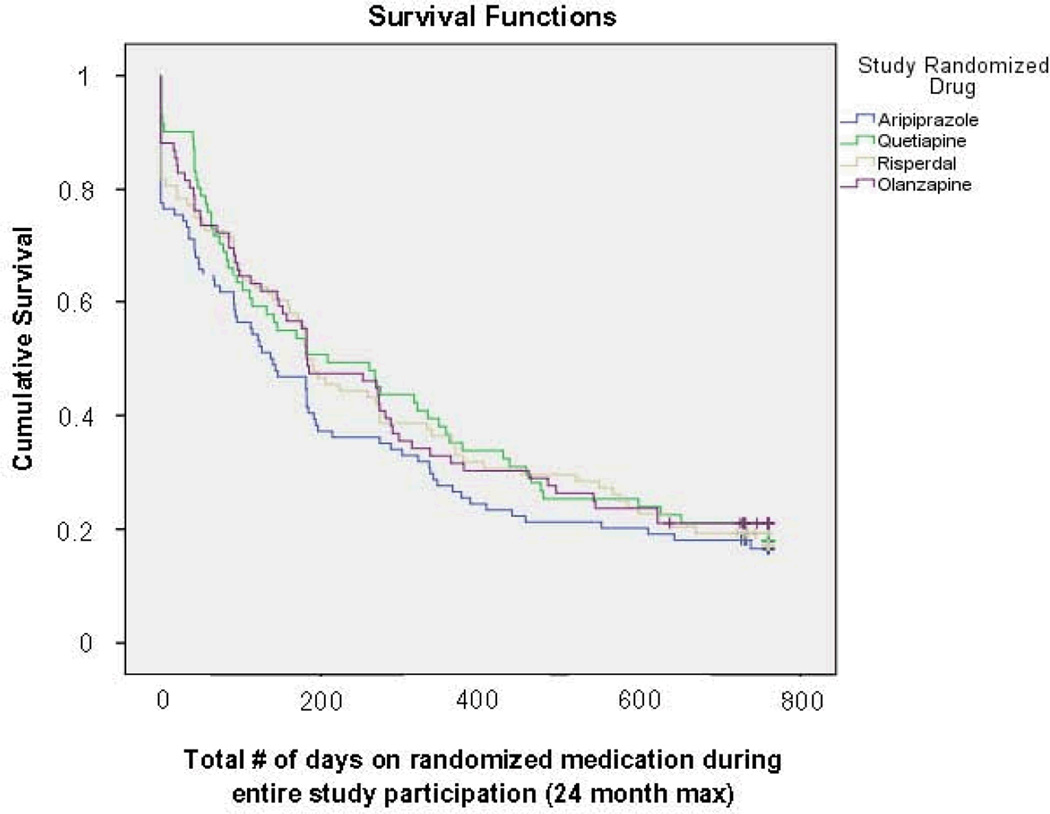
Results: Because of a high incidence of serious adverse events, quetiapine was discontinued midway through the trial. There were significant differences among patients willing to be randomized to different atypical antipsychotics (P < .01), suggesting that treating clinicians tended to exclude olanzapine and prefer aripiprazole as one of the possible choices in patients with metabolic problems. Yet, the atypical antipsychotic groups did not differ in longitudinal changes in metabolic parameters or on most other outcome measures. Overall results suggested a high discontinuation rate (median duration 26 weeks prior to discontinuation), lack of significant improvement in psychopathology, and high cumulative incidence of metabolic syndrome (36.5% in 1 year) and of serious (23.7%) and nonserious (50.8%) adverse events for all atypical antipsychotics in the study.
Conclusions: Employing a study design that closely mimicked clinical practice, we found a lack of effectiveness and a high incidence of side effects with 4 commonly prescribed atypical antipsychotics across diagnostic groups in patients over age 40, with relatively few differences among the drugs. Caution in the use of these drugs is warranted in middle-aged and older patients.
Trial registration: ClinicalTrials.gov identifier: NCT00245206.
© Copyright 2013 Physicians Postgraduate Press, Inc.
Conflict of interest statement
Hua Jin, MD. Conflict of Interest Disclosure: He and his spouse have had no relevant financial interests or personal affiliations during at least the past 12 months.
Pei-an Betty Shih, PhD. Conflict of Interest Disclosure: She and her spouse have had no relevant financial interests or personal affiliations during at least the past 12 months.
Shahrokh Golshan, PhD. Conflict of Interest Disclosure: He and his spouse have had no relevant financial interests or personal affiliations during at least the past 12 months.
Sunder Mudaliar, MD. Conflict of Interest Disclosure: He is a Consultant and on the Speaker's Bureau for Astra-Zeneca and Bristol Myers Squibb which manufacture the drugs used in this study.
Robert Henry, MD. Conflict of Interest Disclosure: He and his spouse/partner have had no relevant financial interests or personal affiliations during at least the past 12 months.
Danielle K. Glorioso, MSW. Conflict of Interest Disclosure: She and her spouse have had no relevant financial interests or personal affiliations during at least the past 12 months.
Stephan Arndt, PhD. Conflict of Interest Disclosure: He and his spouse/partner have had no relevant financial interests or personal affiliations during at least the past 12 months.
Helena C. Kraemer, PhD. Conflict of Interest Disclosure: She and her spouse have had no relevant financial interests or personal affiliations during at least the past 12 months.
Dilip V. Jeste, MD. Conflict of Interest Disclosure: He and his spouse have had no relevant financial interests or personal affiliations during at least the past 12 months.
Figures
Comment in
-
No better solution for antipsychotic treatment with regard to long-term safety and effectiveness.Evid Based Ment Health. 2015 Feb;18(1):17. doi: 10.1136/eb-2014-101801. Epub 2014 Sep 19. Evid Based Ment Health. 2015. PMID: 25239248 Free PMC article. No abstract available.
Similar articles
-
A randomized trial examining the effectiveness of switching from olanzapine, quetiapine, or risperidone to aripiprazole to reduce metabolic risk: comparison of antipsychotics for metabolic problems (CAMP).Am J Psychiatry. 2011 Sep;168(9):947-56. doi: 10.1176/appi.ajp.2011.10111609. Epub 2011 Jul 18. Am J Psychiatry. 2011. PMID: 21768610 Free PMC article. Clinical Trial.
-
A multicenter, randomized, double-blind, placebo-controlled, 16-week study of adjunctive aripiprazole for schizophrenia or schizoaffective disorder inadequately treated with quetiapine or risperidone monotherapy.J Clin Psychiatry. 2009 Oct;70(10):1348-57. doi: 10.4088/JCP.09m05154yel. J Clin Psychiatry. 2009. PMID: 19906340 Clinical Trial.
-
Adjunctive effects of aripiprazole on metabolic profiles: comparison of patients treated with olanzapine to patients treated with other atypical antipsychotic drugs.Prog Neuropsychopharmacol Biol Psychiatry. 2013 Jan 10;40:260-6. doi: 10.1016/j.pnpbp.2012.10.010. Epub 2012 Oct 18. Prog Neuropsychopharmacol Biol Psychiatry. 2013. PMID: 23085073
-
Efficacy and safety of atypical antipsychotic drugs (quetiapine, risperidone, aripiprazole and paliperidone) compared with placebo or typical antipsychotic drugs for treating refractory schizophrenia: overview of systematic reviews.Sao Paulo Med J. 2010 May;128(3):141-66. doi: 10.1590/s1516-31802010000300007. Sao Paulo Med J. 2010. PMID: 20963366 Free PMC article. Review.
-
Efficacy of atypical antipsychotics in elderly patients with dementia.J Clin Psychiatry. 2004;65 Suppl 11:11-5. J Clin Psychiatry. 2004. PMID: 15264966 Review.
Cited by
-
Simulated Effects of Policies to Reduce Diabetes Risk Among Adults With Schizophrenia Receiving Antipsychotics.Psychiatr Serv. 2017 Dec 1;68(12):1280-1287. doi: 10.1176/appi.ps.201500485. Epub 2017 Sep 1. Psychiatr Serv. 2017. PMID: 28859580 Free PMC article.
-
Late-onset schizophrenia: do recent studies support categorizing LOS as a subtype of schizophrenia?Curr Opin Psychiatry. 2014 May;27(3):173-8. doi: 10.1097/YCO.0000000000000049. Curr Opin Psychiatry. 2014. PMID: 24613985 Free PMC article. Review.
-
Additional Comments.Dtsch Arztebl Int. 2017 Nov 3;114(44):753. doi: 10.3238/arztebl.2017.0753a. Dtsch Arztebl Int. 2017. PMID: 29169434 Free PMC article. No abstract available.
-
Treating older adults with schizophrenia: challenges and opportunities.Schizophr Bull. 2013 Sep;39(5):966-8. doi: 10.1093/schbul/sbt043. Epub 2013 Apr 3. Schizophr Bull. 2013. PMID: 23552180 Free PMC article.
-
Metabolomics Biomarkers for Precision Psychiatry.Adv Exp Med Biol. 2019;1161:101-113. doi: 10.1007/978-3-030-21735-8_10. Adv Exp Med Biol. 2019. PMID: 31562625 Free PMC article. Review.
References
-
- Jeste DV, Dolder CR. Treatment of non-schizophrenic disorders: Focus on atypical antipsychotics. J Psychiat Research. 2003;38:73–103. - PubMed
-
- Jeste DV, Alexopoulos GS, Bartels SJ, et al. Consensus statement on the upcoming crisis in geriatric mental health: Research agenda for the next two decades. Arch Gen Psychiatry. 1999;56:848–853. - PubMed
-
- Alexopoulos GS, Streim JE, Carpenter D. Expert consensus guidelines for using antipsychotic agents in older patients. J Clin Psychiatry. 2004;65:5–99. - PubMed
-
- McDonald WM, Wermager J. Pharmacologic treatment of geriatric mania. Curr Psychiatry Rep. 2002;4:43–50. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
- R01 MH106781/MH/NIMH NIH HHS/United States
- M01RR 000827/RR/NCRR NIH HHS/United States
- TL1 RR031979/RR/NCRR NIH HHS/United States
- P30MH080002-01/MH/NIMH NIH HHS/United States
- MH071536/MH/NIMH NIH HHS/United States
- 1K01DK087813-01/DK/NIDDK NIH HHS/United States
- P30 MH080002/MH/NIMH NIH HHS/United States
- UL1RR031980/RR/NCRR NIH HHS/United States
- M01 RR000827/RR/NCRR NIH HHS/United States
- R01 MH071536/MH/NIMH NIH HHS/United States
- K01 DK087813/DK/NIDDK NIH HHS/United States
- UL1 RR031980/RR/NCRR NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
