

Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial
- PMID: 23219286
- PMCID: PMC3596060
- DOI: 10.1016/S0140-6736(12)61963-1
Long-term effects of continuing adjuvant tamoxifen to 10 years versus stopping at 5 years after diagnosis of oestrogen receptor-positive breast cancer: ATLAS, a randomised trial
Erratum in
- Lancet. 2013 Mar 9;381(9869):804
-
Department of Error.Lancet. 2017 May 13;389(10082):1884. doi: 10.1016/S0140-6736(17)31004-8. Epub 2017 Apr 28. Lancet. 2017. PMID: 28457627 Free PMC article. No abstract available.
Abstract
Background: For women with oestrogen receptor (ER)-positive early breast cancer, treatment with tamoxifen for 5 years substantially reduces the breast cancer mortality rate throughout the first 15 years after diagnosis. We aimed to assess the further effects of continuing tamoxifen to 10 years instead of stopping at 5 years.
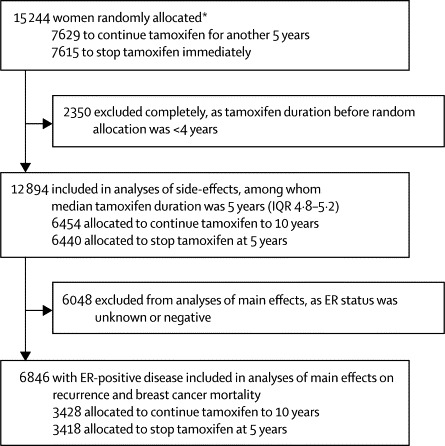
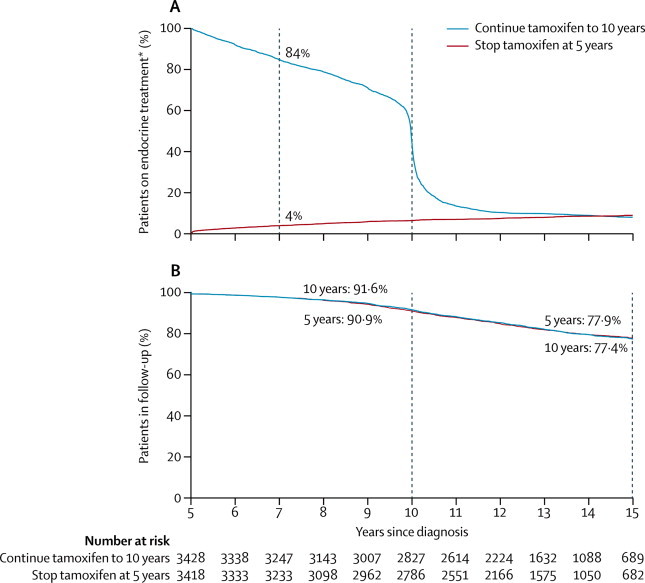
Methods: In the worldwide Adjuvant Tamoxifen: Longer Against Shorter (ATLAS) trial, 12,894 women with early breast cancer who had completed 5 years of treatment with tamoxifen were randomly allocated to continue tamoxifen to 10 years or stop at 5 years (open control). Allocation (1:1) was by central computer, using minimisation. After entry (between 1996 and 2005), yearly follow-up forms recorded any recurrence, second cancer, hospital admission, or death. We report effects on breast cancer outcomes among the 6846 women with ER-positive disease, and side-effects among all women (with positive, negative, or unknown ER status). Long-term follow-up still continues. This study is registered, number ISRCTN19652633.
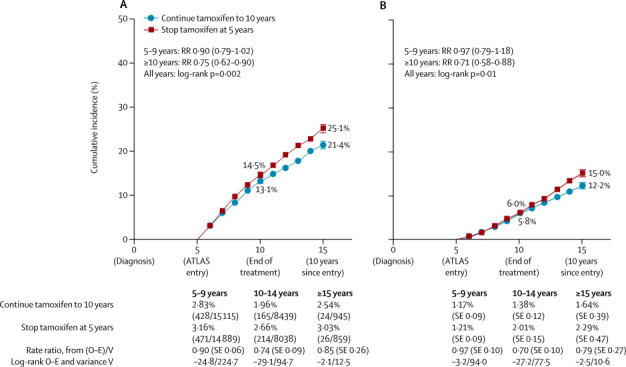
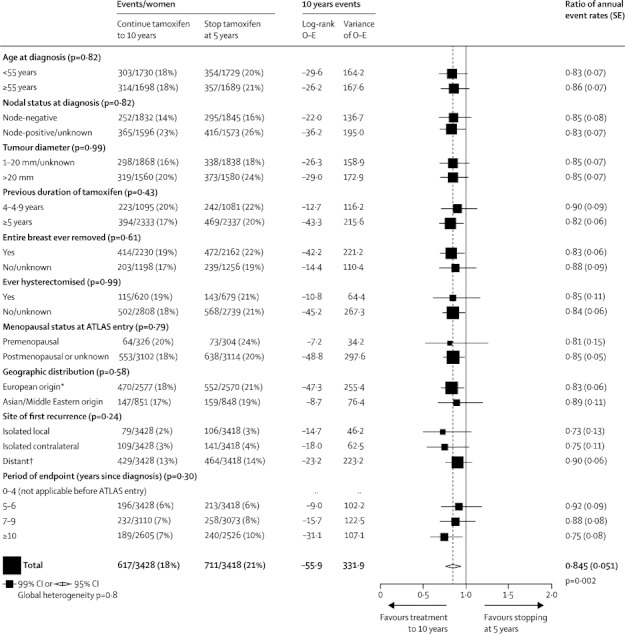
Findings: Among women with ER-positive disease, allocation to continue tamoxifen reduced the risk of breast cancer recurrence (617 recurrences in 3428 women allocated to continue vs 711 in 3418 controls, p=0·002), reduced breast cancer mortality (331 deaths vs 397 deaths, p=0·01), and reduced overall mortality (639 deaths vs 722 deaths, p=0·01). The reductions in adverse breast cancer outcomes appeared to be less extreme before than after year 10 (recurrence rate ratio [RR] 0·90 [95% CI 0·79–1·02] during years 5–9 and 0·75 [0·62–0·90] in later years; breast cancer mortality RR 0·97 [0·79–1·18] during years 5–9 and 0·71 [0·58–0·88] in later years). The cumulative risk of recurrence during years 5–14 was 21·4% for women allocated to continue versus 25·1% for controls; breast cancer mortality during years 5–14 was 12·2% for women allocated to continue versus 15·0% for controls (absolute mortality reduction 2·8%). Treatment allocation seemed to have no effect on breast cancer outcome among 1248 women with ER-negative disease, and an intermediate effect among 4800 women with unknown ER status. Among all 12,894 women, mortality without recurrence from causes other than breast cancer was little affected (691 deaths without recurrence in 6454 women allocated to continue versus 679 deaths in 6440 controls; RR 0·99 [0·89–1·10]; p=0·84). For the incidence (hospitalisation or death) rates of specific diseases, RRs were as follows: pulmonary embolus 1·87 (95% CI 1·13–3·07, p=0·01 [including 0·2% mortality in both treatment groups]), stroke 1·06 (0·83–1·36), ischaemic heart disease 0·76 (0·60–0·95, p=0·02), and endometrial cancer 1·74 (1·30–2·34, p=0·0002). The cumulative risk of endometrial cancer during years 5–14 was 3·1% (mortality 0·4%) for women allocated to continue versus 1·6% (mortality 0·2%) for controls (absolute mortality increase 0·2%).
Interpretation: For women with ER-positive disease, continuing tamoxifen to 10 years rather than stopping at 5 years produces a further reduction in recurrence and mortality, particularly after year 10. These results, taken together with results from previous trials of 5 years of tamoxifen treatment versus none, suggest that 10 years of tamoxifen treatment can approximately halve breast cancer mortality during the second decade after diagnosis.
Funding: Cancer Research UK, UK Medical Research Council, AstraZeneca UK, US Army, EU-Biomed.
Figures
Comment in
-
Extended adjuvant tamoxifen for breast cancer--a new era?Lancet. 2013 Mar 9;381(9869):782-3. doi: 10.1016/S0140-6736(12)62038-8. Lancet. 2013. PMID: 23219287 No abstract available.
-
10 vs 5 years of adjuvant tamoxifen: exclusion of 1/402 centres in ATLAS.Lancet. 2017 May 13;389(10082):1884. doi: 10.1016/S0140-6736(17)31003-6. Epub 2017 Apr 28. Lancet. 2017. PMID: 28457628 No abstract available.
-
Rethinking Extended Adjuvant Antiestrogen Therapy to Increase Survivorship in Breast Cancer.JAMA Oncol. 2018 Jan 1;4(1):15-16. doi: 10.1001/jamaoncol.2017.3510. JAMA Oncol. 2018. PMID: 29145574 No abstract available.
References
-
- Early Breast Cancer Trialists' Collaborative Group (EBCTCG) Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
-
- Swain SM. Tamoxifen: the long and short of it. J Natl Cancer Inst. 1996;88:1510–1512. - PubMed
-
- Peto R. Five years of tamoxifen—or more? J Natl Cancer Inst. 1996;88:1791–1793. - PubMed
-
- Fisher B, Costantino JP, Wickerham DL. Tamoxifen for the prevention of breast cancer: current status of the National Surgical Adjuvant Breast and Bowel Project P-1 study. J Natl Cancer Inst. 2005;97:1652–1662. - PubMed
