

Association of histologic variants in FSGS clinical trial with presenting features and outcomes
- PMID: 23220425
- PMCID: PMC3586971
- DOI: 10.2215/CJN.06100612
Association of histologic variants in FSGS clinical trial with presenting features and outcomes
Abstract
Background and objectives: FSGS histologic variants have correlated with outcomes in retrospective studies. The FSGS Clinical Trial provided a unique opportunity to study the clinical impact of histologic variants in a well defined prospective cohort with steroid-resistant primary FSGS.
Design, setting, participants, & measurements: Renal biopsies of 138 FSGS Clinical Trial participants aged 2-38 years enrolled from 2004 to 2008 were analyzed using the Columbia classification by core pathologists. This study assessed the distribution of histologic variants and examined their clinical and biopsy characteristics and relationships to patient outcomes.
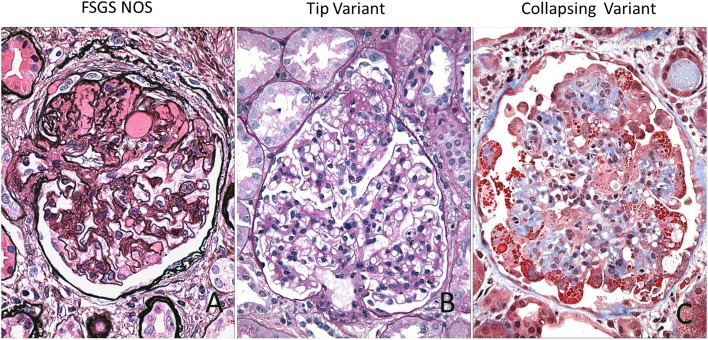
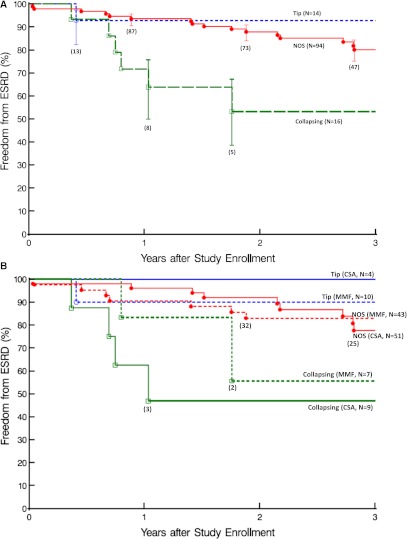
Results: The distribution of histologic variants was 68% (n=94) FSGS not otherwise specified, 12% (n=16) collapsing, 10% (n=14) tip, 7% (n=10) perihilar, and 3% (n=4) cellular. Individuals with not otherwise specified FSGS were more likely to have subnephrotic proteinuria (P=0.01); 33% of teenagers and adults had tip or collapsing variants compared with 10% of children, and subjects with these variants had greater proteinuria and hypoalbuminemia than not otherwise specified patients. Tip variant had the strongest association with white race (86%) and the lowest pathologic injury scores, baseline creatinine, and rate of progression. Collapsing variant had the strongest association with black race (63%, P=0.03) and the highest pathologic injury scores (P=0.003), baseline serum creatinine (P=0.003), and rate of progression. At 3 years, 47% of collapsing, 20% of not otherwise specified, and 7% of tip variant patients reached ESRD (P=0.005).
Conclusions: This is the first prospective study with protocol-defined immunomodulating therapies confirming poor renal survival in collapsing variant and showing better renal survival in tip variant among steroid-resistant patients.
Figures
Comment in
-
Glomerular disease: association of FSGS histologic variants with patient outcomes.Nat Rev Nephrol. 2013 Feb;9(2):65. doi: 10.1038/nrneph.2012.272. Epub 2013 Jan 8. Nat Rev Nephrol. 2013. PMID: 23296292 No abstract available.
-
Histologic classification of FSGS: does form delineate function?Clin J Am Soc Nephrol. 2013 Mar;8(3):344-6. doi: 10.2215/CJN.00660113. Epub 2013 Feb 21. Clin J Am Soc Nephrol. 2013. PMID: 23430205 No abstract available.
References
-
- Gipson DS, Trachtman H, Kaskel FJ, Greene TH, Radeva MK, Gassman JJ, Moxey-Mims MM, Hogg RJ, Watkins SL, Fine RN, Hogan SL, Middleton JP, Vehaskari VM, Flynn PA, Powell LM, Vento SM, McMahan JL, Siegel N, D’Agati VD, Friedman AL: Clinical trial of focal segmental glomerulosclerosis in children and young adults. Kidney Int 80: 868–878, 2011 - PMC - PubMed
-
- Gipson DS, Trachtman H, Kaskel FJ, Radeva MK, Gassman J, Greene TH, Moxey-Mims MM, Hogg RJ, Watkins SL, Fine RN, Middleton JP, Vehaskari VM, Hogan SL, Vento S, Flynn PA, Powell LM, McMahan JL, Siegel N, Friedman AL: Clinical trials treating focal segmental glomerulosclerosis should measure patient quality of life. Kidney Int 79: 678–685, 2011 - PMC - PubMed
-
- D’Agati VD, Fogo AB, Bruijn JA, Jennette JC: Pathologic classification of focal segmental glomerulosclerosis: A working proposal. Am J Kidney Dis 43: 368–382, 2004 - PubMed
-
- Stokes MB, Valeri AM, Markowitz GS, D’Agati VD: Cellular focal segmental glomerulosclerosis: Clinical and pathologic features. Kidney Int 70: 1783–1792, 2006 - PubMed
-
- Thomas DB, Franceschini N, Hogan SL, Ten Holder S, Jennette CE, Falk RJ, Jennette JC: Clinical and pathologic characteristics of focal segmental glomerulosclerosis pathologic variants. Kidney Int 69: 920–926, 2006 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
