

Innate immune function and mortality in critically ill children with influenza: a multicenter study
- PMID: 23222256
- PMCID: PMC3705720
- DOI: 10.1097/CCM.0b013e318267633c
Innate immune function and mortality in critically ill children with influenza: a multicenter study
Abstract
Objective: To prospectively evaluate relationships among serum cytokine levels, innate immune responsiveness, and mortality in a multicenter cohort of critically ill children with influenza infection.
Design: Prospective, multicenter, observational study.
Setting: Fifteen pediatric ICUs among members of the Pediatric Acute Lung Injury and Sepsis Investigators network.
Patients: Patients ≤18 yrs old admitted to a PICU with community-acquired influenza infection. A control group of outpatient children was also evaluated.
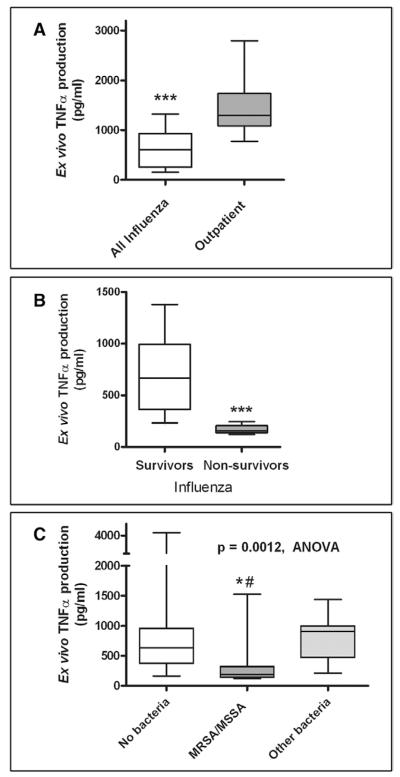
Interventions: ICU patients underwent sampling within 72 hrs of ICU admission for measurement of a panel of 31 serum cytokine levels and quantification of whole blood ex vivo lipopolysaccharide-stimulated tumor necrosis factor-α production capacity using a standardized stimulation protocol. Outpatient control subjects also underwent measurement of tumor necrosis factor-α production capacity.
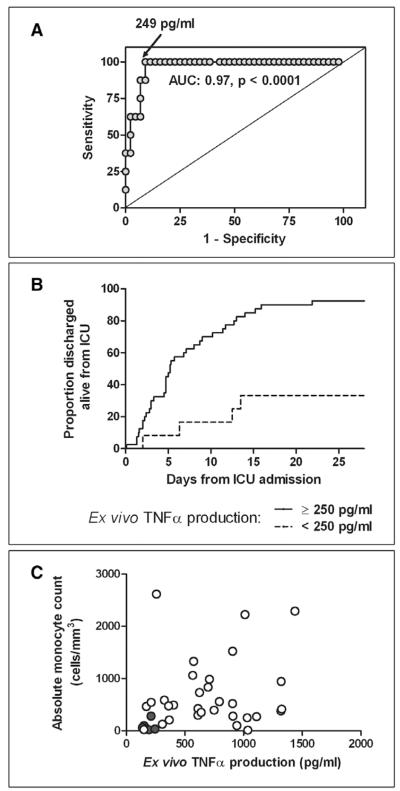
Measurements and main results: Fifty-two patients (44 survivors, eight deaths) were sampled. High levels of serum cytokines (granulocyte macrophage colony-stimulating factor, interleukin-6, interleukin-8, interferon-inducible protein-10, monocyte chemotactic protein-1, and macrophage inflammatory protein-1α) were associated with mortality (p < 0.0016 for each comparison) as was the presence of secondary infection with Staphylococcus aureus (p = 0.007), particularly methicillin-resistant S. aureus (p < 0.0001). Nonsurvivors were immunosuppressed with leukopenia and markedly reduced tumor necrosis factor-α production capacity compared with outpatient control subjects (n = 21, p < 0.0001) and to ICU survivors (p < 0.0001). This association remained after controlling for multiple covariables. A tumor necrosis factor-α response <250 pg/mL was highly predictive of death and longer duration of ICU stay (p < 0.0001). Patients with S. aureus coinfection demonstrated the greatest degree of immunosuppression (p < 0.0001).
Conclusions: High serum levels of cytokines can coexist with marked innate immune suppression in children with critical influenza. Severe, early innate immune suppression is highly associated with both S. aureus coinfection and mortality in this population. Multicenter innate immune function testing is feasible and can identify these high-risk children.
Figures
Comment in
-
Dysfunction of the innate immune system during sepsis: a call for research.Crit Care Med. 2013 Jan;41(1):364-5. doi: 10.1097/CCM.0b013e318270e57b. Crit Care Med. 2013. PMID: 23269155 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
