

Tolerance induction in HLA disparate living donor kidney transplantation by donor stem cell infusion: durable chimerism predicts outcome
- PMID: 23222893
- PMCID: PMC3531567
- DOI: 10.1097/TP.0b013e3182782fc1
Tolerance induction in HLA disparate living donor kidney transplantation by donor stem cell infusion: durable chimerism predicts outcome
Abstract
Background: We recently reported that durable chimerism can be safely established in mismatched kidney recipients through nonmyeloablative conditioning followed by infusion of a facilitating cell (FC)-based hematopoietic stem cell transplantation termed FCRx. Here we provide intermediate-term follow-up on this phase II trial.
Methods: Fifteen human leukocyte antigen-mismatched living donor renal transplant recipients underwent low-intensity conditioning (fludarabine, cyclophosphamide, 200 cGy TBI), received a living donor kidney transplant on day 0, then infusion of cryopreserved FCRx on day +1. Maintenance immunosuppression, consisting of tacrolimus and mycophenolate, was weaned over 1 year.
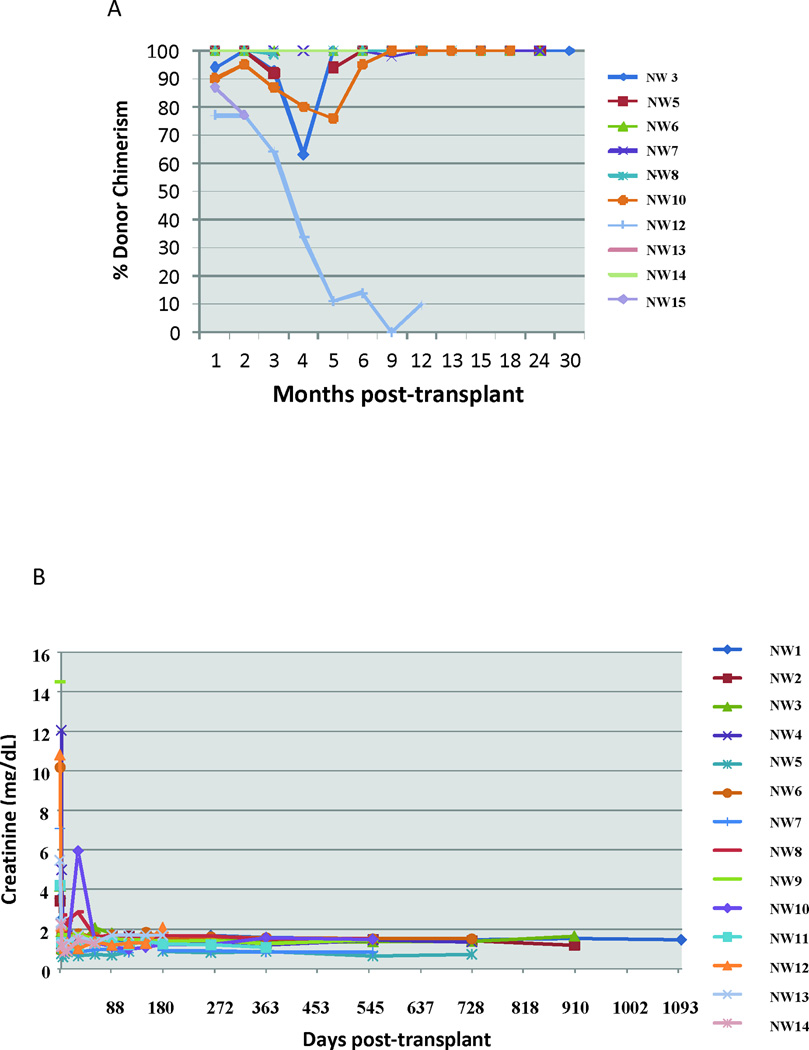
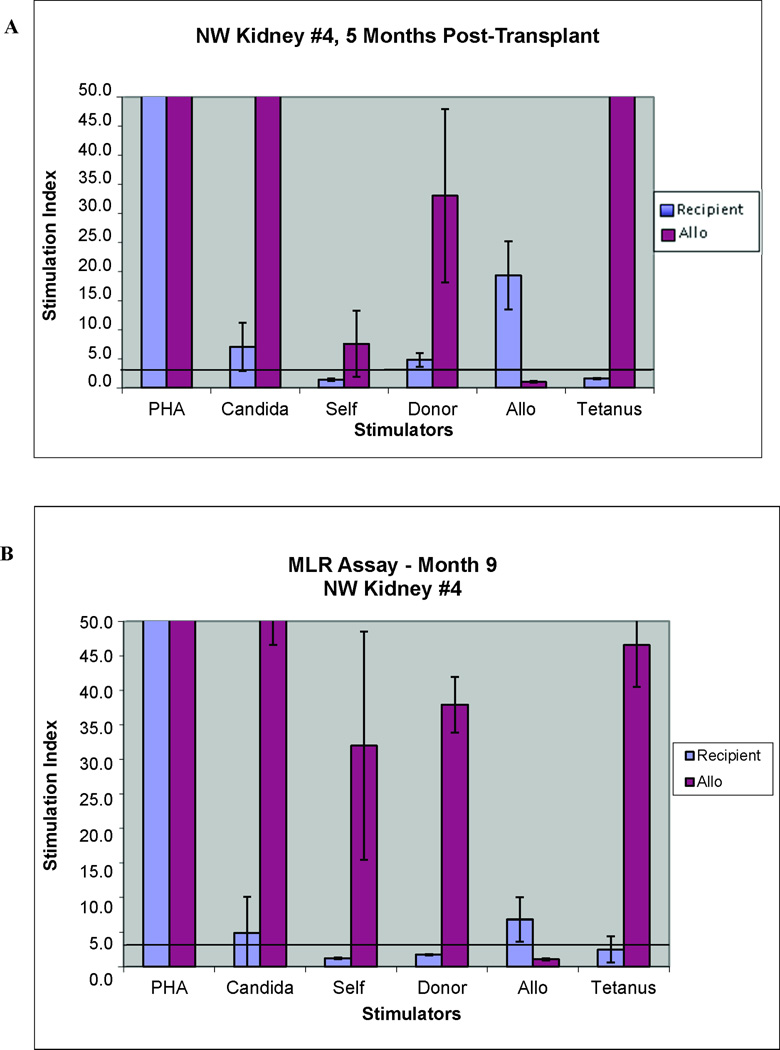
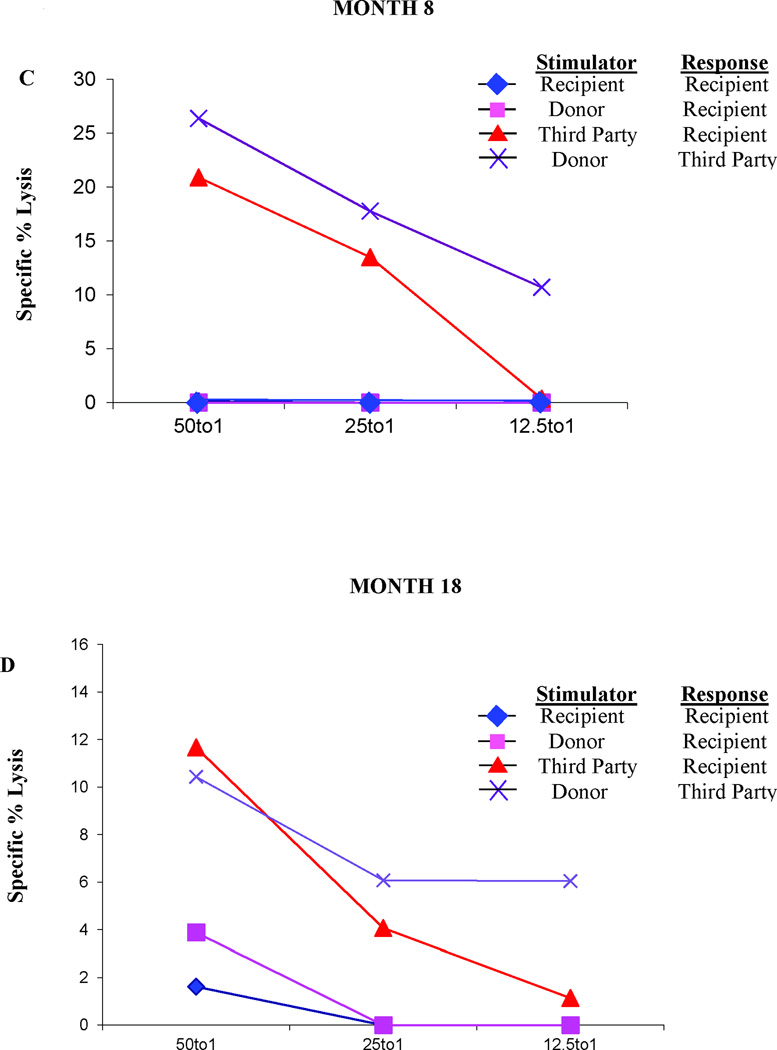
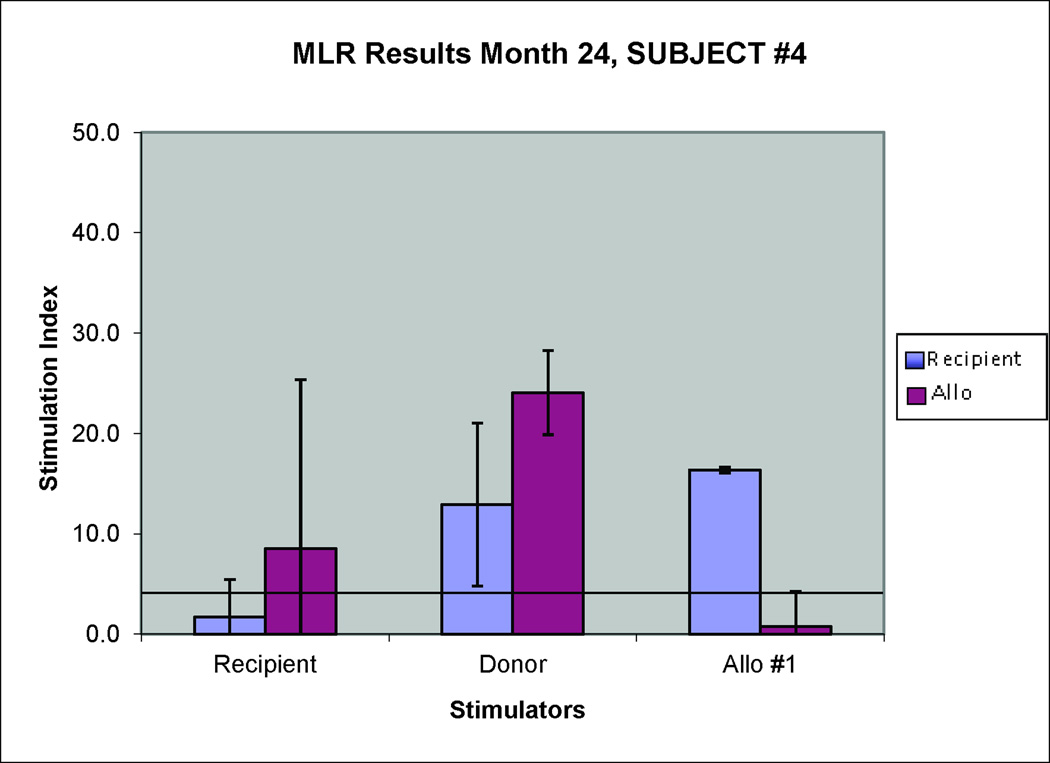
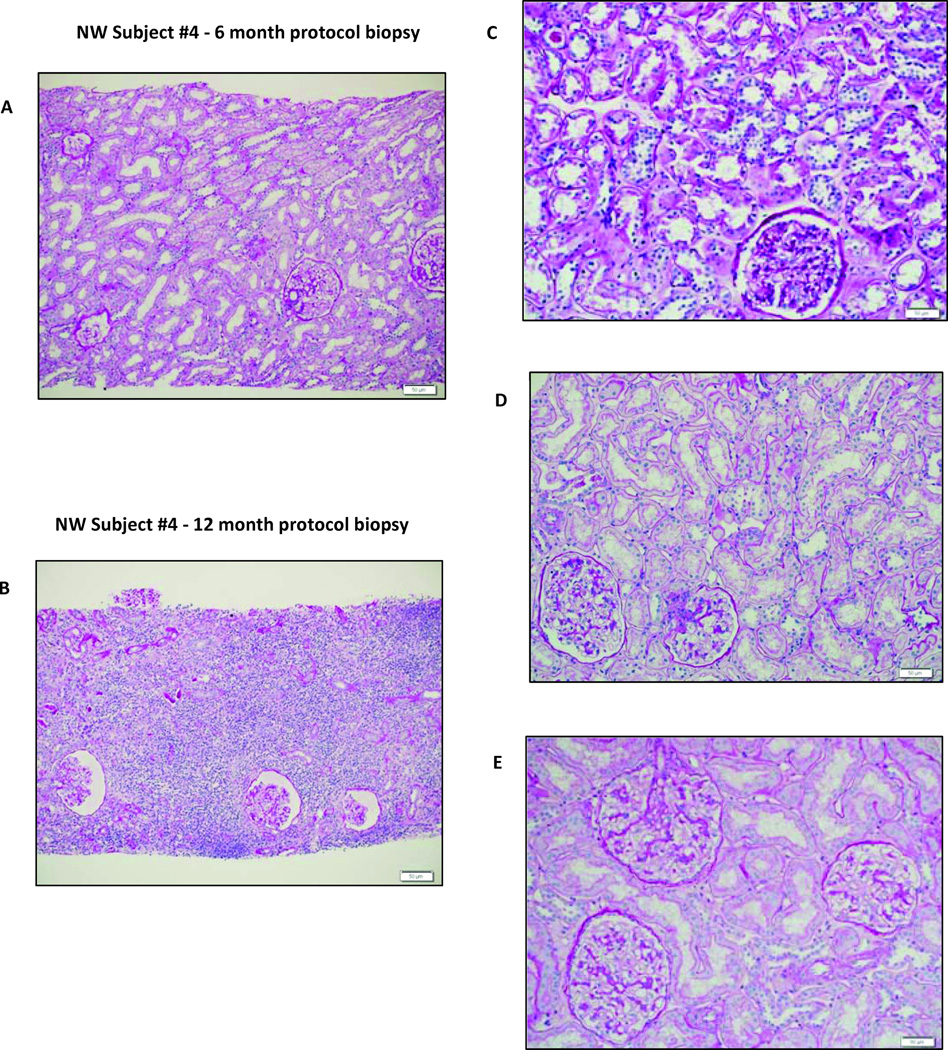
Results: All but one patient demonstrated peripheral blood macrochimerism after transplantation. Engraftment failure occurred in a highly sensitized (panel reactive antibody [PRA] of 52%) recipient. Chimerism was lost in three patients at 2, 3, and 6 months after transplantation. Two of these subjects had received either a reduced cell dose or incomplete conditioning; the other two had PRA greater than 20%. All demonstrated donor-specific hyporesponsiveness and were weaned from full-dose immunosuppression. Complete immunosuppression withdrawal at 1 year after transplantation was successful in all patients with durable chimerism. There has been no graft-versus-host disease or engraftment syndrome. Renal transplantation loss occurred in one patient who developed sepsis following an atypical viral infection. Two subjects with only transient chimerism demonstrated subclinical rejection on protocol biopsy despite donor-specific hyporesponsiveness.
Conclusions: Low-intensity conditioning plus FCRx safely achieved durable chimerism in mismatched allograft recipients. Sensitization represents an obstacle to successful induction of chimerism. Sustained T-cell chimerism is a more robust biomarker of tolerance than donor-specific hyporeactivity.
Figures
References
-
- Owen RD. Immunogenetic consequences of vascular anastomoses between bovine twins. Science. 1945;102:400. - PubMed
-
- Billingham RE, Brent L, Medawar PB. Actively acquired tolerance to foreign cells. Nature. 1953;172:603. - PubMed
-
- Feng S, Ekong UD, Lobritto SJ, et al. Complete immunosuppression withdrawal and subsequent allograft function among pediatric recipients of parental living donor liver transplants. JAMA. 2012;307:283. - PubMed
-
- Levitsky J. Operational tolerance: past lessons and future prospects. Liver Transpl. 2011;17:222. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
