

Birt-Hogg-Dube syndrome: clinicopathological features of the lung
- PMID: 23223565
- PMCID: PMC3595143
- DOI: 10.1136/jclinpath-2012-201200
Birt-Hogg-Dube syndrome: clinicopathological features of the lung
Abstract
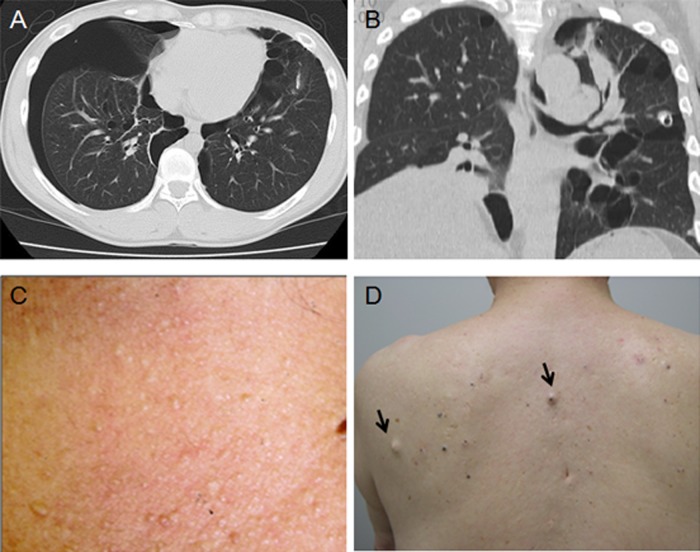
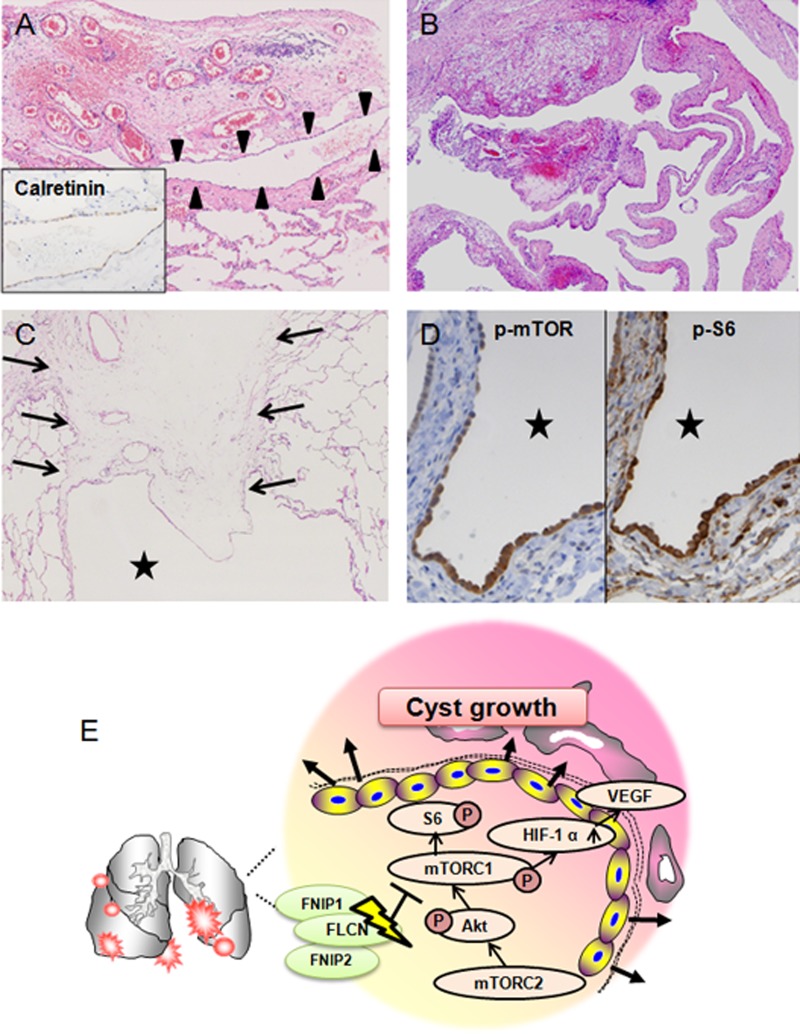
Birt-Hogg-Dubé syndrome (BHD) is an autosomal dominant inherited disorder characterised by fibrofolliculomas, renal tumours, pulmonary cysts and pneumothorax. The pulmonary cysts and repeated episodes of pneumothorax are the clinical hallmarks for discovering families affected by the syndrome. This disorder is caused by mutations in the gene coding for folliculin (FLCN). FLCN forms a complex with FLCN-interacting protein 1 (FNIP1) and FNIP2 (also known as FNIPL), and the complex cross-talks with signalling molecules such as 5'-AMP-activated protein kinase (AMPK) and the mammalian target of rapamycin (mTOR). Heterozygous Flcn knockout mice and rats with Flcn gene mutations develop renal cysts, adenomas and/or carcinomas. These findings suggest that FLCN functions as a tumour suppressor that inhibits renal carcinogenesis. However, the mechanisms of the formation of pulmonary cysts and pneumothorax associated with heterozygous mutations in FLCN are poorly understood. Resected lung specimens from patients with BHD are often misdiagnosed by pathologists as non-specific blebs or bullae or emphysema, and patients with BHD who have pulmonary cysts and repeated pneumothorax frequently do not receive appropriate medical investigations. This review discusses the clinical and pathological features of lungs of patients with BHD, focusing on the diagnostic pathology and possible mechanisms of cyst formation.
Figures


References
-
- Birt AR, Hogg GR, Dube WJ. Hereditary multiple fibrofolliculomas with trichodiscomas and acrochordons. Arch Dermatol 1977;113:1674–7 - PubMed
-
- Hornstein OP, Knickenberg M. Perifollicular fibromatosis cutis with polyps of the colon: a cutaneo-intestinal syndrome sui generis. Arch Dermatol Res 1975;253:161–75 - PubMed
-
- Happle R. Hornstein-Birt-Hogg-Dube syndrome: a renaming and reconsideration. Am J Med Genet A 2012;158A:1247–51 - PubMed
-
- Khoo SK, Bradley M, Wong FK, et al. Birt-Hogg-Dube syndrome: mapping of a novel hereditary neoplasia gene to chromosome 17p12-q11.2. Oncogene 2001;20:5239–42 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous